9
“I would like to point out that in the history of
medicine, there are many examples of situations
where the vast majority of physicians did something
that turned out to be wrong. The best example is
bloodletting, which was the most common medical
practice from the first century A.D. until the
nineteenth century.”
—NASSIR GHAEMI, TUFTS MEDICAL CENTER,
APA CONFERENCE (2008)
At the American Psychiatric Association’s 2008 annual meeting in Washington, D.C., there were press conferences each day, and during the presentations that told of the great advances that lay ahead, the leaders of the APA regularly urged the reporters and science writers in attendance to help “get out the message that [psychiatric] treatment works and is effective, and that our diseases are real diseases just like cardiovascular diseases and cancer,” said APA president Carolyn Robinowitz. “We need to work together as partners so we can get the word out to patients and families.” The press had an important role to play, explained incoming president Nada Logan Stotland, because “the public is vulnerable to misinformation.” She urged the reporters to “help us inform the public that psychiatric illnesses are real, psychiatric treatments work, and that our data is as solid as in other areas of medicine.”
I scribbled all of these quotes in my notebook, even though it didn’t seem that Anatomy of an Epidemic was going to quite fit the partnership model that the APA had in mind, and then each day I would go for a stroll in the great exhibit hall, which I always enjoyed. Eli Lilly, Pfizer, Bristol-Myers Squibb, and the other leading vendors of psychiatric drugs all had huge welcoming centers, where, if you were a doctor, you could collect various trinkets and gifts. Pfizer’s seemed to be the most popular, as the psychiatrists could pick up a new personalized gift each day, their names printed on a mini-flashlight one day and a mobile phone charger the next. They could also win a gift by playing a video game called the Physician’s Race Challenge, the pace of their virtual self racing toward the finish line governed by how well they answered questions about the wonders of Geodon as a treatment for bipolar illness. After playing that game, many lined up to have their photo taken and stamped on a campaign button that said: “Best Doctor on Earth.”
The best-attended events of the conference were the industry-sponsored symposiums. At every breakfast, lunch, and dinner hour, the doctors could enjoy a sumptuous free meal, which was then followed by talks on the chosen topic. There were symposiums on depression, ADHD, schizophrenia, and the prescribing of antipsychotics to children and adolescents, and nearly all of the speakers hailed from top academic schools. The fact that they all were being paid by the drug companies was openly acknowledged, as the APA, as part of a new disclosure policy, had published a chart listing all the ways that pharmaceutical money flowed to these “thought leaders.” In addition to receiving research monies, most of the “experts” served as consultants, on “advisory boards,” and as members of “speakers’ bureaus.” Thus, you could see that Joseph Biederman, a psychiatrist at Massachusetts General Hospital in Boston who, during the 1990s, led the way in popularizing juvenile bipolar disorder, received research grants from eight firms, acted as a “consultant” to nine, and served as a “speaker” for eight. His long list of pharmaceutical clients was not all that unusual, and at times, speakers had to update their information in the disclosure guide when they strode to the podium, as they had recently added yet another pharmaceutical company to their list of clients. After Harvard Medical School’s Jean Frazier dutifully relayed such information, at a symposium devoted to the merits of putting children on multiple psychiatric drugs, she said, without any apparent hint of irony, “I hope you find my presentation unbiased.”
The speakers put on very polished presentations, evidence of the training in public speaking they had received from the pharmaceutical firms. They regularly opened with a joke before moving on to their PowerPoint slides, which were splashed on ballroom screens larger than those found in most theaters. Often the diners were given handheld remote devices to answer multiple-choice questions during the presentations, with dramatic music playing as they keyed in their responses, much as it might during “Final Jeopardy,” and when their collective wisdom was splashed on the screens, most usually got the answer right. “You guys are so smart,” one speaker said.
Patty Duke provided the 2008 APA meeting with its celebrity patient story. AstraZeneca sponsored her talk, and the company spokesman who introduced her, apparently worried that somehow the audience might miss the point of what she had to say, informed everyone that “the take-home message is that mental illness is diagnosable and recognizable, and that treatment works.” Then the Oscar-winning actress, clad in a pumpkin orange dress, told of how she had suffered from undiagnosed bipolar illness for twenty years, during which time she drank excessively and was sexually promiscuous. Diagnosis and medication “made me marriage material,” she said, and whenever she speaks to patient groups around the country, she hammers this point home. “I tell them, ‘Take your medicines!’” she said. The drugs fix the disease “with very little downside!” The audience clapped loudly at that, and then America’s favorite identical cousin offered the psychiatrists a final benediction: “We are beyond blessed to have people like you who have chosen to take care of us and to lead us to a balanced life…. I get my information from you and NAMI [National Alliance on Mental Illness], and if I resisted such information, I would deserve to have a net thrown over me. When I hear someone say, at one of my talks, ‘I don’t need the medication, I don’t take it,’ I tell them to ‘sit down, you are making a fool of yourself.’”
That led to a standing ovation, and so, as I put away my notebook, it seemed certain that this was a meeting where the bottomline message, no matter where you went, would be quite well controlled. Nearly everything was set up and organized in a way that told of a profession quite confident in its therapeutics, and while I knew that Martin Harrow would be giving a talk on his long-term study of schizophrenia outcomes, he had been allotted only twenty minutes, and his session had been assigned to one of the convention center’s smallest rooms. His presentation would be the one exception to the rule, and so I didn’t expect to hear anything startling on the Tuesday afternoon that I squeezed my way into a crowded, slightly larger room for a forum titled “Antidepressants in Bipolar Disorder.” I figured that the speakers would simply present trial results that justified, in one way or another, the use of these drugs, but soon I was writing furiously away. The discussion, which was led by the top bipolar experts in the country, including the two grand old men of biological psychiatry in the United States, Frederick Goodwin and Robert Post, focused on this question: Do anti-depressants worsen the long-term course of bipolar disorder? And notably so?
“The illness has been altered,” said Goodwin, who in 1990 coauthored the first edition of his text Manic-Depressive Illness, which is considered the bible in the field. Today “we have a lot more rapid cycling than we described in the first edition, a lot more mixed states than we described in the first edition, a lot more lithium resistance, and a lot more lithium treatment failure than there was in the first edition. The illness is not what Kraepelin described anymore, and the biggest factor, I think, is that most patients who have the illness get an antidepressant before they ever get exposed to a mood stabilizer.”
This was the opening salvo in what turned into an hour-long confessional. Although not all the speakers agreed that antidepressants had been disastrous for bipolar patients, that was the general theme, and nobody questioned Goodwin’s bottom-line summary that bipolar outcomes had noticeably worsened in the past twenty years. Antidepressants, said Nassir Ghaemi, from Tufts Medical Center, can cause manic switches and turn patients into “rapid cyclers,” and may increase the amount of time they spend in depressive episodes. Rapid cycling, Post added, led to a very bad end.
“The number of episodes, and it’s a very rich literature [documenting this], is associated with more cognitive deficits,” he said. “We are building more episodes, more treatment resistance, more cognitive dysfunction, and there is data showing that if you have four depressive episodes, unipolar or bipolar, it doubles your late-life risk of dementia. And guess what? That isn’t even the half of it…. In the United States, people with depression, bipolar, and schizophrenia are losing twelve to twenty years in life expectancy compared to people not in the mental health system.”
These were words that told of a paradigm of care that had completely failed, of treatment that made patients constantly symptomatic and cognitively impaired, and led to their early death as well. “Now you just heard that one of the things we do doesn’t work very well in the long term,” Post practically screamed. “So what the hell should we be doing?”
The confessions came fast and furious. Psychiatry, of course, had its “evidence base” for using antidepressants in bipolar disorder, but, Post said, the clinical trials conducted by pharmaceutical companies “are virtually useless for us as clinicians…. They don’t tell us what we really need to know, what our patients are going to respond to, and if they don’t respond to that first treatment, what should be the next iteration, and how long they should stay on things.” Only a small percentage of people, he added, actually “respond to these crummy treatments, like antidepressants.” As for recent pharma-funded trials that had shown that bipolar patients withdrawn from antipsychotic medications relapsed at high rates, which theoretically served as evidence that patients needed to take these drugs long-term, those studies “were designed to get relapse [in the placebo group],” Goodwin said. “It isn’t evidence that the drug is still needed; it’s evidence that if you suddenly change a brain that has adapted to the drug, you are going to get relapse.” Added Post: “Right now, fifty years after the advent of antidepressant drugs, we still don’t really know how to treat bipolar depression. We need new treatment algorithms that aren’t just made up.”
This was all much like the moment in The Wizard of Oz when the curtain is pulled back and the mighty wizard is revealed as a frail old man. For anyone in the audience who had spent his or her morning in Pfizer’s welcoming center, answering video-game questions about the wonders of Geodon for bipolar illness, it must have been crushing. Thirty years earlier, Guy Chouinard and Barry Jones had rattled the profession with their talks on drug-induced “supersensitivity psychosis,” and now the profession was being asked to confront the fact that bipolar outcomes were worse today than they had been thirty years earlier, and that antidepressants were a likely culprit. Stimulants, it seemed, could make bipolar patients worse too, and at last Ghaemi told the audience that psychiatry needed to adopt a “Hippocratic” approach to the use of psychiatric medications, which would require them to stop prescribing them unless they had good evidence they were truly beneficial over the long term. “Diagnosis, not druggery,” he said, and at one point, several in the audience—which had grown increasingly agitated by this discussion—booed him.
“Can fifty thousand psychiatrists be wrong?” he asked, speaking about the profession’s use of antidepressants as a treatment for bipolar disorder. “I think that the answer is yes, probably.”
Bipolar Before Lithium
Readers of this book, having come this far in the text, cannot be surprised to learn that outcomes for bipolar disorder have dramatically worsened in the pharmacotherapy era. The only surprising thing is that this failure was so openly discussed at the APA meeting. Given what the scientific literature revealed about the long-term outcomes of medicated schizophrenia, anxiety, and depression, it stood to reason that the drug cocktails used to treat bipolar illness were not going to produce good long-term results. The increased chronicity, the functional decline, the cognitive impairment, and the physical illness—all of these can be expected to show up in people treated with a cocktail that often includes an antidepressant, an antipsychotic, a mood stabilizer, a benzodiazepine, and perhaps a stimulant, too. This was a medical train wreck that could have been anticipated, and unfortunately, as we trace the history of this story, the details will seem all too familiar.
Although “bipolar” illness is a diagnosis of recent origin, first showing up in the APA’s Diagnostic and Statistical Manual in 1980 (DSM-III), medical texts dating back to Hippocrates contain descriptions of patients suffering from alternating episodes of mania and melancholia. “Melancholia,” wrote German physician Christian Vater in the seventeenth century, “often passes into mania and vice versa. The melancholics now laugh, now are saddened, now express numberless other absurd gestures and forms of behaviour.” The English mad doctor John Haslam told of how “the most furious maniacs suddenly sink into a profound melancholy, and the most depressed and miserable objects become violent and raving.” In 1854, a French asylum doctor, Jules Baillarger, dubbed this illness la folie à double forme. It was an uncommon, but recognizable form of insanity.1
When Emil Kraepelin published his diagnostic texts, he put these patients into his manic-depressive group. This diagnostic category also included patients who suffered from depression or mania only (as opposed to both), and Kraepelin reasoned that these varied emotional states all arose from the same underlying disease. The splitting of manic-depressive disorder into separate unipolar and bipolar factions got its start in 1957, when a German psychiatrist, Karl Leonhard, determined that the manic form of the illness seemed to run more in families than the depressive form did. He called the manic patients “bipolar,” and other researchers then identified additional differences between the unipolar and bipolar forms of manic-depressive illness. Onset occurred earlier in bipolar patients, often when they were in their twenties, and it also appeared that bipolar patients were at somewhat higher risk of becoming chronically ill.
In his 1969 book, Manic Depressive Illness, George Winokur at Washington University in St. Louis treated unipolar depression and bipolar illness as separate entities, and with this distinction having been made, he and others began reviewing the literature on manic-depressive illness to isolate the data on the “bipolar” patients. On average, in the older studies, about one-fourth of the manic-depressive group had suffered from manic episodes and thus were “bipolar.” By all accounts, this was a rare disorder. There were perhaps 12,750 people hospitalized with bipolar illness in 1955, a disability rate of one in every 13,000 people.2 That year there were only about 2,400 “first admissions” for bipolar illness in the country’s mental hospitals.3
As Winokur discovered, the long-term outcomes of the manic patients in the pre-drug era had been pretty good. In his 1931 study, Horatio Pollock reported that 50 percent of the patients admitted to New York State mental hospitals for a first attack of mania never suffered a second attack (during an eleven-year follow-up), and only 20 percent experienced three or more episodes.4 F. I. Wertham, from Johns Hopkins Medical School, in a 1929 study of two thousand manic-depressive patients, determined that 80 percent of the manic group recovered within a year, and that fewer than 1 percent required long-term hospitalization.5 In Gunnar Lundquist’s study, 75 percent of the 103 manic patients recovered within ten months, and during the following twenty years, half of the patients never had another attack, and only 8 percent developed a chronic course. Eighty-five percent of the group “socially recovered” and resumed their former positions.6 Finally, Ming Tsuang, at the University of Iowa, studied how eighty-six manic patients admitted to a psychiatric hospital between 1935 and 1944 fared over the next thirty years, and he found that nearly 70 percent had good outcomes, which meant they married, lived in their own homes, and worked. Half were asymptomatic during this lengthy follow-up. All in all, the manic patients had fared as well as the unipolar patients in Tsuang’s study.7
These results, Winokur wrote, revealed that there “was no basis to consider that manic depressive psychosis permanently affected those who suffered from it. In this way it is, of course, different from schizophrenia.” While some people suffered multiple episodes of mania and depression, each episode was usually only “a few months in duration,” and “in a significant number of patients, only one episode of illness occurs.” Most important of all, once patients recovered from their bipolar episodes, they usually had “no difficulty resuming their usual occupations.”8
Gateways to Bipolar
Today, according to the NIMH, bipolar illness affects one in every forty adults in the United States, and so, before we review the outcomes literature for this disorder, we need to try to understand this astonishing increase in its prevalence.9 Although the quick-and-easy explanation is that psychiatry has greatly expanded the diagnostic boundaries, that is only part of the story. Psychotropic drugs—both legal and illegal—have helped fuel the bipolar boom.
In studies of first-episode bipolar patients, investigators at McLean Hospital, the University of Pittsburgh, and the University of Cincinnati Hospital found that at least one-third had used marijuana or some other illegal drug prior to their first manic or psychotic episode.10 This substance abuse, the University of Cincinnati investigators concluded, may “initiate progressively more severe affective responses, culminating in manic or depressive episodes, that then become self-perpetuating.”11 Even the one-third figure may be low; in 2008, researchers at Mt. Sinai Medical School reported that nearly two-thirds of the bipolar patients hospitalized at Silver Hill Hospital in Connecticut in 2005 and 2006 experienced their first bout of “mood instability” after they had abused illicit drugs.12 Stimulants, cocaine, marijuana, and hallucinogens were common culprits. In 2007, Dutch investigators reported that marijuana use “is associated with a fivefold increase in the risk of a first diagnosis of bipolar disorder” and that one-third of new bipolar cases in the Netherlands resulted from it.13
Antidepressants have also led many people into the bipolar camp, and to understand why, all we have to do is return to the discovery of this class of drugs. We see tuberculosis patients treated with iproniazid dancing in the wards, and while that magazine report was probably a bit exaggerated, it told of lethargic patients suddenly behaving in a manic way. In 1956, George Crane published the first report of antidepressant-induced mania, and this problem has remained present in the scientific literature ever since.14 In 1985, Swiss investigators tracking changes in the patient mix at Burghölzli psychiatric hospital in Zurich reported that the percentage with manic symptoms jumped dramatically following the introduction of antidepressants. “Bipolar disorders increased; more patients were admitted with frequent episodes,” they wrote.15 In a 1993 practice guide to depression, the APA confessed that “all anti-depressant treatments, including ECT [electroconvulsive therapy], may provoke manic or hypomanic episodes.”16 A few years later, researchers at Yale University School of Medicine quantified this risk. They reviewed the records of 87,290 patients diagnosed with depression or anxiety between 1997 and 2001 and determined those treated with antidepressants converted to bipolar at the rate of 7.7 percent per year, which was three times greater than for those not exposed to the drugs.17 As a result, over longer periods, 20 to 40 percent of all patients initially diagnosed with unipolar depression today eventually convert to bipolar illness.18 Indeed, in a recent survey of members of the Depressive and Manic-Depressive Association, 60 percent of those with a bipolar diagnosis said they had initially fallen ill with major depression and had turned bipolar after exposure to an antidepressant.19
This is data that tells of a process that routinely manufactures bipolar patients. “If you create iatrogenically a bipolar patient,” explained Fred Goodwin, in a 2005 interview in Primary Psychiatry, “that patient is likely to have recurrences of bipolar illness even if the offending antidepressant is discontinued. The evidence shows that once a patient has had a manic episode, he or she is more likely to have another one, even without the antidepressant stimulation.”20 Italy’s Giovanni Fava put it this way: “Antidepressant-induced mania is not simply a temporary and fully reversible phenomenon, but may trigger complex biochemical mechanisms of illness deterioration.”21
With illegal and legal drugs greasing the road to bipolar illness, it is little wonder that a rare disorder in 1955 has become commonplace today. SSRIs took the country by storm in the 1990s, and from 1996 to 2004, the number of adults diagnosed with bipolar illness rose 56 percent. At the same time, psychiatry’s steady expansion of diagnostic boundaries over the past thirty-five years has helped fuel the bipolar boom too.
When bipolar disorder was first separated from manic-depressive illness, the diagnosis required a person to have suffered bouts of mania and depression so severe that each type had resulted in hospitalization. Then, in 1976, Goodwin and others at the NIMH suggested that if a person had been hospitalized for depression but not for mania, and yet had experienced a mild episode of mania (hypomania), he or she could be diagnosed with bipolar II, a less severe form of the disease. Then the bipolar II diagnosis was expanded so that it included people who had never been hospitalized for either depression or mania, but simply had experienced episodes of both. Next, in the 1990s, the psychiatric community decided that a diagnosis of hypomania no longer required four days of “elevated, expansive, or irritable mood,” but rather simply two days of such moodiness. Bipolar illness was on the march, and with the diagnostic boundaries expanded in this way, researchers were suddenly announcing that it affected up to 5 percent of the population. But even that didn’t end the bipolar boom: In 2003, former NIMH director Lewis Judd and others argued that many people suffer “subthreshold” symptoms of depression and mania, and thus could be diagnosed with “bipolar spectrum disorder.”22 There was now bipolar I, bipolar II, and a “bipolarity intermediate between bipolar disorder and normality,” one bipolar expert explained.23Judd calculated that 6.4 percent of American adults suffer from bipolar symptoms; others have argued that one in every four adults now falls into the catchall bipolar bin, this once-rare illness apparently striking almost as frequently as the common cold.24
The Lithium Years
With the psychopharmacology revolution in full bloom during the 1960s, it seemed that every major psychiatric disorder should have its own magic bullet, and once bipolar disorder was separated from manic-depressive illness, psychiatry found a suitable candidate in lithium. Salts made from this alkali metal had been hanging around the fringes of medicine for more than 150 years, and then suddenly, during the early 1970s, lithium was touted as a cure of sorts for this newly identified disease. “I have not found another treatment in psychiatry that works so quickly, so specifically, and so permanently as lithium for recurrent manic and depressive mood states,” said Columbia University psychiatrist Ronald Fieve, in his 1975 book, Moodswing.25
Nature’s lightest metal, lithium was discovered in 1818, found in rocks off the Swedish coast. It was reported to dissolve uric acid and thus was marketed as a therapy that could break up kidney stones and the uric crystals that gathered in the joints of people who suffered from gout. In the late 1800s and early 1900s, lithium became a popular ingredient in elixirs and tonics, and it would even be added to beers and other beverages. However, lithium was eventually found to have no uric-acid–dissolving properties, and in 1949, the FDA banned it after it was found to cause cardiovascular problems.26
Its revival as a psychiatric drug began in Australia, where the physician John Cade fed it to guinea pigs and observed that it made them docile. In 1949, he reported that he had successfully treated ten manic patients with lithium; however, he neglected to mention in his published article that the treatment killed one person and made two others severely ill. As makers of lithium tonics had long known, lithium can be toxic even in fairly small doses. Both intellectual function and motor movement may become impaired, and if too high of a dose is given, a person may lapse into a coma and die.
As a group, psychiatrists in the United States showed little interest in lithium until bipolar made its appearance as a distinct illness. Prior to that time, Thorazine and other neuroleptics were used to curb manic episodes and thus there was no need for another drug that seemed to have similar brain-dampening effects. But once George Winokur published his book in 1969 dividing manic-depressive illness into unipolar and bipolar forms, psychiatry had a new disease in need of its own antidote.
Since no pharmaceutical company could patent lithium, the APA took the lead in getting the FDA to approve it. Only a few placebo-controlled trials of the drug were ever conducted. In 1985, UK researchers who scoured the scientific literature could only find four of any merit. However, in those studies, lithium produced a good response in 75 percent of the patients, which was much higher than the response rate in the placebo group.27 The second part of the evidence base for lithium came, as usual, from withdrawal studies. Investigators who analyzed nineteen such trials in 1994 found that 53.5 percent of the patients withdrawn from lithium relapsed, versus 37.5 percent of the lithium-maintained patients. That was taken as evidence that lithium prevented relapse, although the researchers noted that in the few studies where patients had been gradually withdrawn from the drug, only 29 percent relapsed (which was lower than the rate among the drug-maintained patients).28
All in all, this was not particularly robust evidence that lithium benefited patients, and during the 1980s, several investigators began raising concerns about its long-term effects. They noted that readmission rates for mania in both the United States and the United Kingdom had risen since lithium was introduced, and eventually it became clear why bipolar patients were turning up at hospital emergency rooms with such great frequency.
Various studies found that more than 50 percent of lithium-treated patients would quit taking the drug in fairly short order, usually because they objected to how the drug dulled their minds and slowed their physical movements, and when they did, they relapsed at astonishingly high rates. In 1999, Ross Baldessarini reported that half of all patients relapsed within five months of quitting lithium, even though in the absence of exposure to the drug, it took nearly three years for 50 percent of bipolar patients to relapse. The time between episodes following lithium withdrawal was seven times shorter than it was naturally.29 “The risk of recurrence after discontinuation of lithium therapy … especially of mania, is much higher than predicted by a patient’s course before treatment or by general knowledge of the natural history of the illness,” Baldessarini wrote.30 Other investigators noted the same phenomenon: “Manic relapse is readily triggered [by lithium withdrawal], probably by the release of supersensitized receptors or membrane pathways,” explained Jonathan Himmelhoch from the University of Pittsburgh.31
This meant that bipolar patients who were treated with lithium and then stopped taking it ended up “worse than if they had never had any drug treatment,” wrote UK psychiatrist Joanna Moncrieff.32 A Scottish psychiatrist, Guy Goodwin, concluded in 1993 that if patients were exposed to lithium and then quit taking it within the first two years, the risk of relapse was so great that the drug may be “harmful to bipolar patients.” The higher hospitalization readmission rates for bipolar patients since the introduction of lithium “could be explained entirely” by this drug-induced worsening, he said.33
Yet the patients who stayed on lithium weren’t faring particularly well either. Roughly 40 percent relapsed within two years of their initial hospitalization, and by the end of five years, more than 60 percent fell sick again.34 There was a core group of good, long-term lithium responders—perhaps 20 percent of those initially treated with the drug—but for the majority of patients, it provided little long-term relief. In 1996, Martin Harrow and Joseph Goldberg, from the University of Illinois, reported that at the end of 4.5 years, 41 percent of the patients on lithium had “poor outcomes,” nearly one-half had been rehospitalized, and as a group they weren’t “functioning” any better than those not taking the drug.35 This was a dismal finding, and then Michael Gitlin at UCLA reported similar five-year results for his lithium-treated bipolar patients. “Even aggressive pharmacological maintenance treatment does not prevent relatively poor outcome in a significant number of bipolar patients,” he wrote.36
Although lithium is still in use today, it lost its place as a first-line therapy once “mood stabilizers” were brought to the market in the late 1990s. As Moncrieff wrote in 1997, summing up lithium’s record of efficacy: “There are indications that it is ineffective in the long-term outlook of bipolar disorders, and it is known to be associated with various forms of harm.”37
Bipolar All the Time
There are really two narratives to be dug out of the scientific literature regarding the treatment of bipolar illness with psychiatric drugs. The first tells of lithium’s rise and fall as a magic bullet for the disorder. The second tells of how bipolar outcomes have dramatically worsened during the psychopharmacology era, with experts in the field documenting this at every turn.
As early as 1965, before lithium had made its triumphant entry into American psychiatry, German psychiatrists were puzzling over the change they were seeing in their manic-depressive patients. Patients treated with antidepressants were relapsing frequently, the drugs “transforming the illness from an episodic course with free intervals to a chronic course with continuous illness,” they wrote. The German physicians also noted that in some patients, “the drugs produced a destabilization in which, for the first time, hypomania was followed by continual cycling between hypomania and depression.”38
This was obviously alarming, for the good outcomes in manic-depressive patients arose from the fact that they spent a large part of their lives in symptom-free intervals between episodes, during which time they functioned well. Antidepressants were destroying those asymptomatic interludes, or at least dramatically shortening them. Prior to the drug era, Kraepelin and others reported that only about one-third of manic patients suffered three or more episodes in their lives. Yet studies of bipolar patients in the 1960s and 1970s told of two-thirds who were becoming chronically ill. “The administration of tricyclics may account for artificially high relapse rate estimates,” Fred Goodwin wrote in 1979. “Induction of mania, break down of otherwise long episodes into multiple ones … induction of rapid cycling … are some of the mechanisms by which the administration of tricyclics may contribute to an increase in the number of episodes.”39
Once again, it was becoming apparent that psychiatric medications were worsening the course of a mental illness. In 1983, Athanasious Koukopoulos, director of a mood disorders clinic in Rome, said that he and his colleagues were observing the same thing in their Italian patients. “The general impression of clinicians today is that the course of recurrences of manic-depressive illness has substantially changed in the last 20 years,” he wrote. “The recurrences of many patients have become more frequent. One sees more manias and hypomanias … more rapid cyclers, and more chronic depressions.” Whereas in the pre-drug era rapid cyclers were unknown, 16 percent of Koukopoulos’s manic-depressive patients were now in this predicament, and they were suffering an astonishing 6.5 mood episodes annually, up from less than one episode a year prior to being treated with an antidepressant. “It certainly seems paradoxical,” he admitted, “that a treatment that is therapeutic for depression can worsen the further course of the disease.”40
In spite of such information, antidepressants continued to be prescribed to bipolar patients, and even today, 60 to 80 percent are exposed to an SSRI or some other antidepressant. As a result, investigators have continued to document the harm done. In 2000, Nassir Ghaemi reported that in a study of thirty-eight bipolar patients treated with an antidepressant, 55 percent developed mania (or hypomania) and 23 percent turned into rapid cyclers. This antidepressant-treated group also spent “significantly more time depressed” than a second group of bipolar patients who weren’t exposed to this class of medication.41 “There are significant risks of mania and long-term worsening with antidepressants,” Ghaemi wrote a few years later, repeating a message that had been uttered many times before.42 At the University of Louisville, Rif El-Mallakh similarly concluded that antidepressants may “destabilize the illness, leading to an increase in the number of both manic and depressive episodes.” The drugs, he added, “increase the likelihood of a mixed state,” in which feelings of depression and mania occur simultaneously.43
In 2003, Koukopoulos chimed in again, reporting that antidepressant-induced rapid cycling fully abates in only one-third of patients over the long term (even after the offending anti depressant is withdrawn), and that 40 percent of patients continue to “cycle rapidly with unmodified severity” for years on end.44 Soon, in 2005, El-Mallakh pointed out yet another problem: Antidepressants could induce a “chronic, dysphoric, irritable state” in bipolar patients, meaning that they were almost continually depressed and miserable.45 Finally, in 2008, in a large NIMH study called the Systematic Treatment Enhancement Program for Bipolar Disorder (STEP-BD), “the major predictor of worse outcome was antidepressant use, which about 60 percent of patients received,” Ghaemi noted.46 The antidepressant users were nearly four times more likely than the non-exposed patients to develop rapid cycling, and twice as likely to have multiple manic or depressive episodes.47 “This study,” wrote Ghaemi, in an editorial that appeared in the American Journal of Psychiatry, “may be one more nail in the coffin of antidepressant use in bipolar disorder.”
During the past ten years, several large studies have documented just how constantly symptomatic bipolar patients are today. In a long-term follow-up of 146 bipolar I patients who enrolled in an NIMH study in 1978–81, Lewis Judd found that they were depressed 32 percent of the time, manic or hypomanic 9 percent of the time, and suffering from mixed symptoms 6 percent of the time.48 The bipolar II patients in that study arguably fared even worse: They were depressed 50 percent of the time. “The nature of this deceptively ‘milder’ form of manic-depressive illness is so chronic as to seem to fill the entire life,” Judd wrote.49 Russell Joffe, at the New Jersey Medical School, reported in 2004 that 33 percent of the bipolar I patients and 22 percent of the bipolar II patients he studied were rapid cyclers, and both groups were symptomatic nearly half of the time.50Meanwhile, Robert Post announced that nearly two-thirds of the 258 bipolar patients he studied had four or more episodes per year.51
All of these studies showed the same bottom-line result: “It is now well established that bipolar disorders are chronic, with a course characterized by frequent affective episode recurrence,” Judd said.52
The Harm Done
In a 2000 paper published in the Psychiatric Quarterly, a Harvard Medical School psychiatrist, Carlos Zarate, and a psychiatrist who worked for Eli Lilly, Mauricio Tohen, opened up a new line of concern: Bipolar patients today aren’t just much more symptomatic than in the past, they also don’t function as well. “In the era prior to pharmacotherapy, poor outcome in mania was considered a relatively rare occurrence,” Zarate and Tohen wrote. “However, modern outcome studies have found that a majority of bipolar patients evidence high rates of functional impairment.” What, they wondered, could explain “these differences”?53
The remarkable decline in the functional outcomes of bipolar patients is easy to document. In the pre-lithium era, 85 percent of mania patients would return to work or to their “pre-morbid” social role (as a housewife, for example). As Winokur wrote in 1969, most patients had “no difficulty resuming their usual occupations.” But then bipolar patients began cycling through emergency rooms more frequently, employment rates began to decline, and soon investigators were reporting that fewer than half of all bipolar patients were employed or otherwise “functionally recovered.” In 1995, Michael Gitlin at UCLA reported that only 28 percent of his bipolar patients had a “good occupational outcome” at the end of five years.54 Three years later, psychiatrists at the University of Cincinnati announced that only 24 percent of their bipolar patients were “functionally recovered” at the end of one year.55 David Kupfer at the University of Pittsburgh School of Medicine, in a study of 2,839 bipolar patients, discovered that even though 60 percent had attended college and 30 percent had graduated, two-thirds were unemployed.56 “In summary,” wrote Ross Baldessarini in a 2007 review article, “functional status is far more impaired in type I bipolar patients than previously believed, [and] remarkably, there is some evidence that functional outcome in type II bipolar patients may be even worse than in type I.”57
The antidepressants, by increasing the frequency of episodes that bipolar patients suffer, naturally reduce their ability to return to work. But, as has become evident in recent years, the problem runs much deeper than that. One of the hallmarks of manic-depressive illness, dating back to Kraepelin, was that once people recovered from their episodes of mania and depression, they were as smart as they had been before they became ill. As Zarate and Tohen noted in their 2000 paper, “studies conducted prior to 1975 found no consistent findings in cognitive deficits in bipolar patients.” But lithium was known to slow thinking, and suddenly researchers began reassessing this belief. In 1993, NIMH investigators compared cognitive function in bipolar and schizophrenia patients, and they concluded that while the bipolar patients showed signs of impairment, the deficits were “more severe and extensive in schizophrenia.”58
This was something of a glass-half-full finding. You could interpret it to mean that cognitive impairment was not that bad in bipolar patients, or, if you remembered the pre-lithium days, you might wonder why these patients were suddenly showing signs of mental decline. But this was just the beginning salvo of a tragic story. Once lithium monotherapy fell from favor, psychiatrists began to turn to “drug cocktails” to treat their patients, and soon investigators had this to report: “Cognitive impairments [that] exist in schizophrenia and affective disorders … cannot be qualitatively distinguished with sufficient reliability.”59 The degree of impairment in these two illnesses was suddenly converging, and in 2001, Faith Dickerson at the Sheppard Pratt Health System in Baltimore provided a more detailed picture of that convergence. She ran seventy-four medicated schizophrenia patients and twenty-six medicated bipolar patients through a series of tests that assessed forty-one cognitive and social-functioning variables, and found that the bipolar patients were as impaired as the schizophrenia patients on thirty-six of the forty-one measures. There was “a similar pattern of cognitive functioning in patients with bipolar disorder as compared to those with schizophrenia,” she wrote. “On most measures of social functioning, our patients with bipolar disorder were not significantly different from those in the schizophrenia group.”60
After that, reports of significant cognitive decline in bipolar patients seemed to pour in from psychiatric researchers around the globe—English, Swedish, German, Australian, and Spanish investigators all told of it. The Australians reported in 2007 that even when bipolar patients are only mildly symptomatic, they are “neuropsychologically scarred”—impaired in their decision-making skills, their verbal fluency, and their ability to remember things.61 Meanwhile, Spanish investigators, after noting that cognitive function in their bipolar and schizophrenia patients “did not differ over time in any test,” concluded that both groups suffered from dysfunction in the “prefrontal cortex and temporolimbic structures.” They also observed that “the more medications the patients received, the greater the psychosocial functioning impairment.”62* Finally, English researchers who looked at the daily lives of bipolar patients found that more than two-thirds “rarely or never engaged in social activities with friends,” their social lives nearly as impoverished as those diagnosed with schizophrenia.63
This was an astonishing convergence in long-term outcomes between the two diagnostic groups, and while the psychiatrists in the United States and abroad who documented it mostly tried, in their discussion of the phenomenon, to ignore the medication elephant in the room, several did confess that it was possible that psychiatric drugs were to blame. Conventional antipsychotics, said Zarate in one of his papers, “may have a negative impact on the overall course of the illness.”64 Later, he and Tohen wrote that “medication induced changes may be yet another factor in explaining the discrepancies in recovery rates between earlier and more recent studies.” The antidepressants, they noted, might cause a “worsening of the course of illness,” while the antipsychotics might lead to more “depressive episodes” and “lower functional recovery rates.” Cognitive impairment was a primary reason that medicated schizophrenia patients fared so poorly over the long term, they said, and “it has been suggested that drug side effects may in part explain the cognitive deficits in bipolar disorder patients.”65 Baldessarini, in his 2007 review, also acknowledged that “neuropharmacological-neuro-toxic factors” might be causing “cognitive deficits in bipolar disorder patients.” Finally, Kupfer threw one more concern into the mix. He detailed all the physical illnesses that now struck bipolar patients—cardiovascular problems, diabetes, obesity, thyroid dysfunction, etc.—and wondered whether “treatment factors such as toxicity from medications” could be causing these devastating ailments, or at least contributing to them.66
All of these writers put their concerns into a conditional context, stating that the drugs might be causing this mental and physical deterioration in their patients. But it’s easy to see that their hesitancy was scientifically unwarranted. Schizophrenia and manic-depressive illness had been diagnostically born as distinct in kind precisely because those with schizophrenia deteriorated cognitively over time, into dementia, while the manic-depressive group did not.* The convergence in outcomes developed once both groups were treated with similar drug cocktails (which usually included an antipsychotic). “The field is witnessing a convergence of pharmacological approaches to the treatment of schizophrenia and bipolar disorder,” wrote Stephen Stahl, author of Antipsychotics and Mood Stabilizers, in 2005. It was adopting “similar blended treatments for these two disease states.”67 Psychiatric drugs, of course, perturb various neurotransmitter pathways in the brain, and thus once schizophrenia and bipolar patients are on similar drug cocktails, they suffer from similar abnormalities in brain function. The convergence of outcomes in the two groups reflects an iatrogenic process at work: The two groups, apart from whatever “natural” problems they may have, both end up suffering from what could be dubbed “polypharmacy psychiatric drug illness.”
Today, bipolar illness is a far cry from what it once was. Prior to the psychopharmacology era, it had been a rare disorder, affecting perhaps one in ten thousand people. Now it affects one in forty (or by some counts, one in twenty). And even though most patients today—at initial diagnosis—are not nearly as ill as the hospitalized patients of the past, their long-term outcomes are almost incomprehensibly worse. In his 2007 review, Baldessarini even detailed, step by step, this remarkable deterioration in outcomes. In the pre-drug era, there was “recovery to euthymia [no symptoms] and a favorable functional adaptation between episodes.” Now there is “slow or incomplete recovery from acute episodes, continued risk of recurrences, and sustained morbidity over time.” Before, 85 percent of bipolar patients would regain complete “premorbid” functioning and return to work. Now only a third achieve “full social and occupational functional recovery to their own premorbid levels.” Before, patients didn’t show cognitive impairment over the long term. Now they end up nearly as impaired as those with schizophrenia. This all tells of an astonishing medical disaster, and then Baldessarini penned what might be considered a fitting epitaph for the entire psychopharmacology revolution:
Prognosis for bipolar disorder was once considered relatively favorable, but contemporary findings suggest that disability and poor outcomes are prevalent, despite major therapeutic advances.68
The Transformation of Bipolar Disorder in the Modern Era
|
Pre-Lithium Bipolar |
Medicated Bipolar Today |
|
|
Prevalence |
1 in 5,000 to 20,000 |
1 in 20 to 50 |
|
Good long-term functional outcomes |
75% to 90% |
33% |
|
Symptom course |
Time-limited acute episodes of mania and major depression with recovery to euthymia and a favorable functional adaptation between episodes |
Slow or incomplete recovery from acute episodes, continued risk of recurrences, and sustained morbidity over time |
|
Cognitive function |
No impairment between episodes or long-term impairment |
Impairment even between episodes; long-term impairment in many cognitive domains; impairment is similar to what is observed in medicated schizophrenia |
This information is drawn from multiple sources. See in particular Huxley, N. “Disability and its treatment in bipolar disorder patients.” Bipolar Disorders 9 (2007): 183–96.
The Graphic That Tells It All
We are now coming to the close of our examination of the outcomes literature for the major psychiatric disorders (for adults), and a return to Martin Harrow’s fifteen-year study on schizophrenia outcomes brings it to a climactic end. In addition to following schizophrenia patients, Harrow studied a group of eighty-one patients with “other psychotic disorders” that would have been described by Kraepelin as a manic-depressive cohort. There were thirty-seven bipolar and twenty-eight unipolar patients in this group, and the remaining sixteen had various milder psychotic disorders. Nearly half of this group stopped taking psychiatric medications during the study, and thus Harrow really had four groups he followed: schizophrenia patients on and off meds and manic-depressive patients on and off meds. Before we review the results, we can run a quick check of our own thoughts: How should we expect the long-term outcomes of all four groups to stack up?
Go ahead—take out a pencil and jot down what you believe the results will be.
Here are his findings. Over the long term, the manic-depressive patients who stopped taking psychiatric drugs fared pretty well. But their recovery took time. At the end of two years, they were still struggling with their illness. Then they began to improve, and by the end of the study their collective scores fell into the “recovered” category (a score of one or two on Harrow’s global assessment scale). The recovered patients were working at least part-time, they had “acceptable” social functioning, and they were largely asymptomatic. Their outcomes fit with Kraepelin’s understanding of manic-depressive illness.
The manic-depressive patients who stayed on their psychiatric medications did not fare so well. At the end of two years, they remained quite ill, so much so they were now a little bit worse than the schizophrenia patients off meds. Then, over the next two-and-one-half years, while the manic-depressive and schizophrenia patients who were off meds improved, the manic-depressive patients who kept taking their pills did not, such that by the end of 4.5 years, they were doing markedly worse than the schizophrenia off-med group. That disparity remained through the rest of the study, and thus here is how the long-term outcomes stacked up, from best to worst: manic-depressive off meds, schizophrenia off meds, manic-depressive on meds, and then schizophrenia on meds.69
Schizophrenia, of course, has long been the psychiatric diagnosis with the worst long-term prognosis. It is the most severe mental illness that nature has to offer. But in this NIMH-funded study, two groups of medicated patients fared worse than the unmedicated schizophrenia patients. The results tell of a medical treatment gone horribly awry, and yet they do not come as a surprise. Anyone who knew the history of the outcomes literature in psychiatry, a history that began to unfold more than fifty years ago, could have predicted that the outcomes would stack up in this way.
In terms of contributing to our modern-day epidemic of disabling mental illness, the bipolar numbers are staggering. In 1955, there were about 12,750 people hospitalized with bipolar illness. Today, according to the NIMH, there are nearly six million adults in the United States with this diagnosis, and according to researchers at the Johns Hopkins School of Public Health, 83 percent are “severely impaired” in some facet of their lives.70 Bipolar illness is now said to be the sixth leading cause of medical-related disability in the world, right behind schizophrenia, and in the near future, as more and more people are diagnosed with this condition and put on drug cocktails, we can expect that bipolar will climb past schizophrenia and take its place behind major depression as the mental illness that fells the most people in the United States. Such is the fruit, bitter in kind, born from the psychopharmacology revolution.
15-Year Outcomes for Schizophrenia and Manic-Depressive Patients
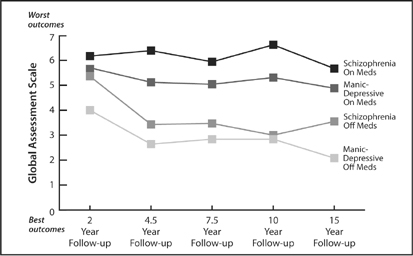
In this graphic, the group labeled “manic depressive” consisted of psychotic patients with bipolar illness, unipolar depression, and milder psychotic disorders. Source: Harrow, M. “Factors involved in outcome and recovery in schizophrenia patients not on antipsychotic medications.” The Journal of Nervous and Mental Disease, 195 (2007): 406–14.
Bipolar Narratives
I interviewed more than sixty people with psychiatric diagnoses for this book, and roughly half at some point had been diagnosed as bipolar. Yet of the thirty or so who got that diagnosis, only four suffered from what might be called “organic” bipolar illness, and that is to say they were hospitalized for a manic episode and had no prior exposure to illicit drugs or antidepressants. Now that we know what science has to tell us about the modern bipolar boom, we can revisit the stories of three people we met in Chapter 2, and see how their stories fit into that story of science. Then we can hear from two people diagnosed with bipolar who, if they had been enrolled in Harrow’s fifteen-year study, would have fallen into his “off-meds” group.
Dorea Vierling-Clausen
If we look at Dorea Vierling-Clausen’s story now, we can see that she has good reason to believe that she should never have been diagnosed with bipolar illness. She went to see a therapist in Denver because she cried too much. She had no history of mania. But then she was prescribed an antidepressant and starting having trouble sleeping, and soon she had a bipolar diagnosis and a prescription for a drug cocktail that included an antipsychotic. A bright teenager had been turned into a mental patient, and Dorea would have continued to be one for the rest of her life if she had not weaned herself from the drugs. When I last spoke to her, in the spring of 2009, she was aglow with the blush of motherhood, as she had recently given birth to a son, Reuben. She and Angela were busily raising their children, with Dorea planning shortly to resume her postdoctoral research at Massachusetts General Hospital, the memory of her “bipolar” days receding into an ever-more-distant past.
Monica Briggs
During the time that I worked on this book, Monica Briggs was the one person who, after an initial interview, got off SSDI (or SSI). She secured a full-time position with the Transformation Center, a peerrun organization in Boston that focuses on helping people “recover” from mental illness, and if you parse her medical story, it’s easy to see that her return to work was related to a change in her medication.
When we first met, I mentioned to Monica the risk of antidepressant-induced mania, and as she remembered back to her breakdown at Middlebury College, a light went on: “I got manic within six weeks of being put on desipramine,” she said. “I’m sure that’s what happened to me.” After that initial manic episode, she was prescribed a drug cocktail that included an antidepressant, and she spent the next twenty years cycling in and out of hospitals, struggling constantly with depression, manic episodes, and suicidal impulses. Psychiatrists put her on eight or nine different antidepressants, and she also went through a series of electroshock treatments. None of this worked. Then, in 2006, she “casually” stopped taking an antidepressant. For the first time, she was on lithium alone, and bingo—the suicidal feelings went away, as did the depression and mania. That symptom relief is what enabled her to work full-time, and now, as she looks back on the horrible twenty years, she is stunned by what she sees: “I have not yet recovered from the immensity of the likelihood that my roulette game with antidepressants exacerbated my illness.”
Steve Lappen
Steve Lappen, who is a leader of the Depressive and Bipolar Support Alliance in Boston, was diagnosed with manic-depressive illness in 1969, when he was nineteen years old. He was one of the four people I interviewed whose manic-depressive illness was “organic” in kind, and on the first day we met, he was in something of a hyper state, talking so fast that I quickly put my pen away and took out a tape recorder instead. “OK,” I told him, “fire away.”
Raised in Newton, Massachusetts, in a family he describes as dysfunctional, Steve got tagged with the “bad apple” label early in life, both by his teachers at school and his parents at home. “I was disruptive in class,” he says. “Every day, during the pledge of allegiance to the flag, I would go sharpen my pencil. I would also get up without provocation and just spin around until I was overcome with dizziness. I would announce that I was a tornado.” He struggled with mood swings even as a kid, and at age sixteen, while hospitalized for fainting spells, he jumped out of bed one night and donned a white coat. “I went around to patient rooms and had conversations as if I were a doctor. I was manic.”
During his first year at Boston College, he was hit by a bout of severe depression. His was a classic case of true manic-depressive illness, and Kraepelin would have recognized the course his illness took over the next five years. “I didn’t take medication,” he explains, and while he suffered several bouts of depression, he did well in between those episodes, particularly when he was in a slightly hypomanic state. “When I was feeling well, I would read more, and I would write papers that weren’t due for two or three months,” he says. “When you are hypomanic, your output is remarkable.” He graduated with a double major in philosophy and English, with nearly a straight-A average.
However, in his first year of graduate school at Stony Brook in Long Island, he had a full-blown manic episode followed by a plunge into depression that left him suicidal. It was then that he was put on lithium and a tricyclic antidepressant for the first time. “I didn’t have mood swings after that, but instead of having a baseline of functioning normally, I was depressed. I was in a state of depression the entire time I was on the medication. I stayed on it for a year and said, ‘No more.’”
Over the next two decades, Steve mostly stayed away from psychiatric medications. He married, had two sons, and divorced. He worked, but skipped from job to job. His life was proceeding down a chaotic path, a chaos that was clearly related to his manic-depressive illness, and yet his life was not marked by vocational disability—he always found work. In 1994, seeking relief from the mood swings that plagued him, he began taking psychiatric medications regularly. He cycled through an endless number of anti-depressants and mood stabilizers, none of which worked for long. Those drug failures led to fourteen electroshock treatments, which in turn left his memory so impaired that when he returned to his job as a financial planner, “I could no longer recognize my best client.” In 1998, he was put on the tricyclic desipramine, which promptly turned him into a rapid cycler. “I’d wake up and feel great, completely emancipated from the demon of depression, and then two days later, I am back into depression,” he explains. “Two days after that, I’m feeling well again. And there is nothing in my external environment that would account for that change in mood.”
He has been on SSDI ever since. The good news is that he hasn’t been hospitalized since 2000, and, as he rightly points out, in spite of his constant battle with bipolar symptoms, he leads a productive life. Remarried now, he volunteers as a “reader” for people who are physically disabled, gives talks about bipolar illness to community groups, and is one of the leaders of DBSA Boston. He also has published essays and poetry in various small publications. But when I last spoke to him, in the spring of 2009, he was cycling through multiple mood swings every day, his symptoms apparently continuing to worsen.
“I would say in the main, I have been worse when taking medication. The medication I am taking now is neutral at best. I wish I could clone myself. I could be my own control group in a trial. I’d like to know if I’d be better, the same, or worse without it.”
Brandon Banks
Brandon Banks can identify the precise moment he became “bipolar,” and while it did involve an antidepressant, there was a series of life events that led up to it. He grew up poor in Elizabethtown, Kentucky, without a father at home, and he has painful memories of sexual abuse, physical abuse, and of a horrible car wreck that killed his aunt, uncle, and another relative. At school, other kids regularly taunted him about a facial birthmark, which so traumatized him that he began wearing a hat pulled low on his head to cover it up. After graduating from high school in 2000, he moved to Louisville, where he went to college part-time and worked nights at United Parcel Service. Soon he noticed that he “wasn’t feeling right,” and when he went back home, his family doctor diagnosed him with “moderate depression” and prescribed an antidepressant. “I went manic in three days,” Brandon says. “It was fast.”
His doctor explained that since he’d had that reaction to the drug, he must be bipolar, rather than just depressed. The drug had “unmasked” the illness, which Brandon took as a positive thing. “I’m thinking, This isn’t so bad, I could have stayed in the system a long time without getting immediate confirmation that I’m bipolar like that.” He was put on a cocktail composed of a mood stabilizer, an antidepressant, and an antipsychotic, and then it hit him. “This was a serious shove into seriousness.”
Over the next four years, his psychiatrists constantly changed his prescriptions. “It was like musical chairs with the cocktails,” he says. “They would tell me, ‘Let’s take this drug out and put this one in.’” He took Depakote, Neurontin, Risperdal, Zyprexa, Seroquel, Haldol, Thorazine, lithium, and an endless succession of antidepressants, and as time went on he became a rapid cycler who suffered from mixed states. His medical records also document the development of new psychiatric symptoms: worsening anxiety, panic attacks, obsessive-compulsive behaviors, voices, hallucinations. He was hospitalized several times, and at one point he climbed up on top of a parking garage and threatened to jump off. His ability to concentrate declined so severely that Kentucky took away his driver’s license. “What my life became was staying at home all day, getting up in the morning and laying my pills out on the counter, taking them, and then going back to sleep because I couldn’t stay awake if I tried. Then I would get up, play some video games, and hang out with my family.”
Twenty-four years old, he felt like a total failure, and one day, after a fight with his mother, he moved out and stopped taking his meds. “I deteriorated badly,” he recalls. “I wasn’t bathing and I wasn’t eating.” However, as the weeks turned into months, his bipolar symptoms lessened, and “I began to think that it’s more like I’m just fucked up,” he says. This was a thought that gave him hope, because now there was the possibility of change, and he took off traveling around the South. “I might as well be homeless,” he told himself, and that journey ultimately turned into a transformative experience. By the time he returned home, he had sworn off eating meat and drinking alcohol, on his way to becoming a “health freak” who practices yoga. “I came back from that trip, and man, I was on top of it. I felt like a million dollars, and everyone in my family—cousins, relatives, aunts and uncles—said that they hadn’t seen me glow like this since I was a kid.”
Since then, Brandon has stayed off psychiatric medications. But it hasn’t been easy, and the up-and-down nature of his life came into sharp relief during his 2008–2009 year at Elizabethtown Community and Technical College. He enrolled there in January of 2008 with dreams of becoming a journalist and a writer, and in the fall, he became managing editor of the school’s newspaper. Under his leadership, the newspaper won twenty-four awards from the Kentucky Intercollegiate Press Association during the 2008–2009 year, and Bran don personally garnered ten such honors for the articles he’d written, including first place in a deadline-writing competition. Incredibly, during those nine months, Brandon racked up other successes too. One of his short stories won second place in a competition and was published in a Louisville weekly; one of his photos was picked as cover art for a literary journal; a short film he shot was nominated for a best documentary award in a local film festival. In May of 2009, his school honored him with its “outstanding sophomore” award. Yet, even during this season of remarkable accomplishment, Brandon suffered several hypomanic and depressive episodes that left him feeling deeply suicidal. “I spent several weekends reading depressive authors with a gun in my hand,” he says. “My accomplishments at these moments just seem to make everything worse. It never seems like enough.”
That is where matters stood in his life in the summer of 2009. He was thriving and struggling at the same time, and his struggles were such that if psychiatric medications had worked for him the first time, he would gladly have turned to them for relief. “I’m still pretty isolated from other people,” he explains. “I stick out because of the birthmark. I’m different. I can’t blend in. It becomes an issue with people. But I’m trying to integrate myself more into life. I have more people in my life now than I have had in a long time. I’m starting to make more contacts. I had lunch with a friend the other day. Doing this is hard for me, and that’s because it’s just not easy for me to deal with people and deal with my emotions. I am trying to get better at it.”
Greg
A math and science whiz, Greg, who asked that I not use his last name, was the sort of child who, when he was in junior high, built a Van de Graaff generator from scrounged parts (which included a vacuum cleaner and a salad bowl, to be precise). However, he had a troubled relationship with his parents, and at the start of his senior year, he began to slide into a mad state (and without having used illegal drugs). “I was delusional, very paranoid, and full of anxiety,” he says. “I was convinced that my parents were trying to kill me.”
Hospitalized for six weeks, Greg was told he was schizoaffective with bipolar tendencies (a “manic-depressive” type diagnosis), and he was discharged on a cocktail composed of two antipsychotics and an antidepressant. But the drugs didn’t chase away his paranoid thoughts, and after he was hospitalized a second time, his psychiatrists added a mood stabilizer and a benzodiazepine to the cocktail and told him he needed to give up his scholastic dreams. “They told me I would be on medication for the rest of my life, and that I would probably be a ward of the state, and that maybe, by the time I was twenty-five or thirty, I could think about getting a part-time job. And I believed it, and so I began trying to figure out how to live with the crushing hopelessness that they are telling you is going to be your life.”
The next five years passed pretty much as his psychiatrists had predicted. Although Greg entered Worcester Polytechnic Institute (WPI) in Massachusetts, he was so heavily medicated that, he says, “I was living in a haze most of the time. Your mind is just a bag of sand. And so I did really poorly in school. I rarely even left my room, and I was kind of out of touch with reality.” He petered along in school for a couple of years, not really making much progress, and then, from 2004 to 2006, he dropped out and mostly stayed in his apartment, smoking marijuana constantly, as “it helped me accept the condition I was forced into.” Six feet, five inches tall, Greg’s weight went from 255 pounds to nearly 500 pounds. “Finally, I said to myself, this is ridiculous. I’d rather be crazy and have a life than not be crazy and not have a life.”
He went for a medical checkup, thinking this would be a first step toward reducing his medications, only to be informed that he needed to stop taking Depakote and Geodon right away, as his liver was shutting down. The abrupt withdrawal induced such physical pain—“sweats, joint and muscle pain, nausea, dizziness,” he says—that he didn’t even pay attention to whether his paranoia was coming back. But in very short order, he was off all of his psychiatric drugs, except for occasional use of a stimulant, and he had also stopped smoking marijuana. “Honestly, it felt like I was waking up for the first time in five years,” he says. “It felt like I had been turned off all those years and had just been rolling through life and I was being pushed around in a wheelchair and finally I had woken up and had gotten back to being myself again. I felt like the drugs took away everything that was me, and then when I went off the drugs, my brain woke up and started working again.”
In late 2007, Greg went back to school. We met in the spring of 2009, and after he had told me the story of his bout with mental illness, he showed me around his research laboratory at WPI, where he now spent eighty hours a week, designing and constructing a robot capable of conducting brain surgery inside an MRI. In a few weeks, he would receive an undergraduate degree in mechanical engineering, and since he’d entered a master’s program while still doing undergraduate work, later that summer he would receive a master’s degree in mechatronics, which is a fusion of mechanical and electrical engineering. The day before my visit, his robotics research had won second prize in a competition that featured 187 entries by graduate students at WPI. Already he had published three papers in academic journals on his project, and in a few weeks he was scheduled to fly to Japan to give a talk about it. He was doing this project under the guidance of a WPI professor, and they expected to conduct animal and cadaver trials with the robot in the fall of 2009. If all went well, clinical trials with humans would begin in two years.
While in his laboratory, Greg showed me the robot and the computer drawings of its circuit boards, which seemed impossibly complex. Naturally, I thought of John Nash, the Princeton mathematician whose inspiring story of recovering from schizophrenia, and doing so while off medication, was told in the book A Beautiful Mind. “I still feel that I have some bad habits to get out of and some better habits to get into before I get into the professional life, but I really do feel that I have left that [mentally ill] part of my life behind,” says Greg, who has lost more than one hundred pounds. “Honestly, I almost never think of it. I now think of myself as a person who is susceptible to building anxiety, but when I start feeling this anxiety, or start feeling negative about things, I stop and say to myself, ‘Are these really reasonable feelings to feel, or is it just insecurity?’ I just have to take the time to check myself.” He is, he concluded, “pretty optimistic about my future now.”
* In this study, the investigators reported that cognitive impairment, from least to most, was as follows, according to drug treatment received: lithium monotherapy, untreated, neuroleptic monotherapy, and then combination drug therapy. However, no details are given about the “untreated” group and whether they had previous exposure to psychiatric medications.
* The schizophrenia patients who routinely deteriorated into dementia were Kraepelin’s dementia praecox patients. That group of patients presented with symptoms very different in kind from schizophrenia patients today, and as we saw in Martin Harrow’s fifteen-year study, many unmedicated schizophrenia patients recover. Courtenay Harding reported the same thing in her long-term study—many of the unmedicated patients had completely recovered. So it’s unclear what percentage of people diagnosed with schizophrenia today, if not continually medicated, would deteriorate cognitively over time.