12
Perhaps the most difficult manifestation of atherosclerotic coronary heart disease to prevent or treat is sudden cardiac arrest (SCA), which describes an abrupt disruption of the heartbeat (arrhythmia) that disables the capacity of the heart to pump blood. This may happen without warning to a seemingly healthy person, who is carrying on his or her normal life one minute and is dead minutes later. Death may come while the unfortunate victim is engaged in strenuous activity, but just as often when he or she is sleeping, reading, watching TV, or even while he is shaving in his hospital room (as was the case for A.L. in Chapter 1). SCA may be the final assault to a damaged or failing heart but is just as often the first and only symptom of a sudden and catastrophic plaque rupture and thrombosis occluding a critical coronary artery in an otherwise healthy heart. According to the 2020 AHA statistical report, which uses data from the Cardiac Arrest Registry to Enhance Survival (CARES), approximately 90% of persons brought to the hospital after suffering an SCA die before leaving the hospital; most are either dead on arrival or die in the emergency room.1 In 2017, there were 379,133 sudden cardia deaths in the U.S. or 97.1 deaths per 100,000. However, nearly half of this total (46%) are of non-cardiac origin (trauma, respiratory failure, etc.), while only 28% are known to be due to heart disease; the remaining 26% are due either to multiple or unknown causes. Thus, if one assumes that half of the SCD with multiple or unknown causes are attributed to heart disease, SCD accounted for about 41% of the 647,457 heart disease deaths in the U.S. in 2017. Only 16% of all SCD (22% of those with a single known cause)—or 21 SCD per 100,000—were due to acute rupture of a coronary plaque. This represents approximately 23% of the 92.9 heart attack deaths per 100,000 in 2017. Thus, the old saw that attributes roughly half of all heart attack deaths to SCD is probably exaggerated.2 But the truth is bad enough.
Whatever the precipitating event, the timeline for responding to sudden cardiac arrest is far shorter than for an “ordinary” myocardial infarction, in which the non-infarcted portion of the heart muscle continues to function. In sudden cardiac arrest, the entire body is suddenly deprived of oxygen—most critically the brain, which can survive for only about 10 minutes in that state. In an ordinary myocardial infarction, the damaged segment of the heart muscle can recover much of its function if the circulation is restored within 3–6 hours. So, given the impossibly short time window for intervention, the only sensible strategy for addressing sudden cardiac arrest is to prevent it; intervening after the fact can only scratch the surface. Prevention of sudden cardiac arrest can be subdivided into primary and secondary prevention. The strategies for primary prevention of sudden cardiac arrest in persons without known cardiovascular disease are the same as those for primary prevention of myocardial infarction and need not be rehearsed here. The same is generally true for secondary prevention in patients without known ventricular dysfunction. So most of this chapter will focus on preventing sudden cardiac arrest in patients with known left ventricular dysfunction.
Let us begin by reviewing how a normal heartbeat is generated and propagates through the heart. Each heart muscle cell contains a metabolic pump that moves potassium ions into the cell and sodium ions out of the cell through specialized channels in the cell membrane. This process creates an electrochemical polarization of the cell membrane, in which the interior has a higher potassium concentration, a lower sodium concentration, and a net negative charge relative to the exterior.3 A heartbeat is initiated by a wave of depolarization that begins in the sinoatrial (SA) node in the right atrium, near the inlet from the superior vena cava, and propagates to the atrioventricular (AV) node near the tricuspid valve between the right atrium and right ventricle, then travels down the ventricular septum via the Bundle of His, which divides into left and right bundle branches which divide into smaller branches that propagate the impulse throughout the left and right ventricles (Figure 12.1).
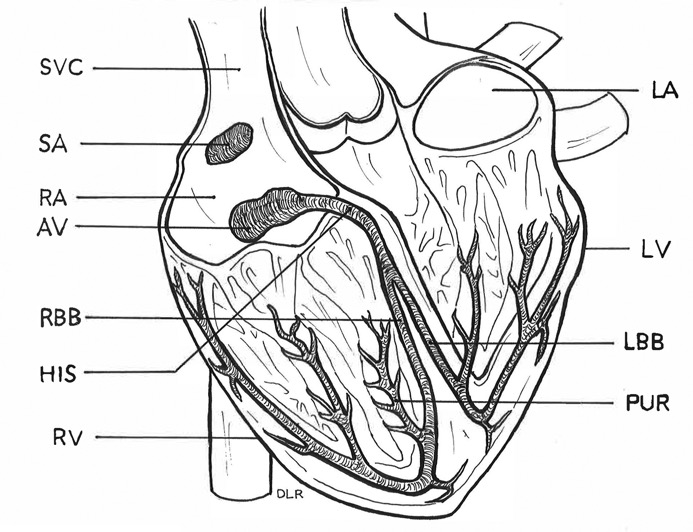
Anatomy of the cardiac conduction system. Drawing by Debra L. Roney. AV = atrioventricular node, HIS = Bundle of His, LA = left atrium, LBB = left bundle branch, LV = left ventricle, PUR = Purkinje fibers, RA = right atrium, RBB—right bundle branch, RV = right ventricle, SA = sinoatrial node, SVC = superior vena cava.
When this electrical wave reaches a heart muscle cell, it momentarily allows sodium to rush into the cell and potassium to rush out, depolarizing the cell membrane and causing the cell (which is packed with filaments of the contractile proteins actin and myosin) to contract. When the wave passes, the cell relaxes and the sodium-potassium pump gets back to work to repolarize the membrane. (This wave of depolarization and repolarization is what an electrocardiogram records.) The ability of the heart to pump blood effectively depends on the ability of the specialized conduction system to generate and propagate regular electrical impulses—60–80 per minute—which permit the heart muscle cells to discharge, contract, and recharge in a coordinated rhythmic fashion.
Any disruption of that rhythmic heartbeat is called an arrhythmia. Arrhythmias originating above the AV node may require an implantable pacemaker or other treatment but do not generally cause sudden cardiac arrest. The most serious of these “supraventricular” arrhythmias is atrial fibrillation (AF), in which the atria do not beat effectively and just allow random impulses to reach the ventricles. The most serious complication of AF is the formation of atrial blood clots, pieces of which may break off and travel to the brain, causing small strokes. Treatments for AF include anticoagulants, drugs that control heart rate (beta-blockers calcium channel blockers, digoxin, etc.) drugs that control rhythm (amiodarone, flecainide, etc.), electrical shock (cardioversion), and surgical or chemical ablation of abnormal sources of electrical impulses.4 But none of this has much to do with heart attack deaths, sudden or otherwise.
From the SCD perspective, ventricular arrhythmias are the problem. Many adults—especially older ones—have the occasional premature ventricular contraction without suffering any ill effects. Impairments of the ventricular conduction system are more serious and may require treatment. However, the lethal ventricular arrhythmias (in order of increasing direness) are ventricular tachycardia (in which the heart beats too rapidly to maintain an adequate BP), ventricular fibrillation (in which the ventricles merely quiver without pumping blood), and asystole (in which electrical activity has ceased); these are the arrhythmias that cause SCA.
Since at least one in every five heart attack deaths presents as sudden death without prior warning, the best way to reduce the toll of SCD—at least the portion that is due to atherosclerotic coronary artery disease—is to prevent the underlying coronary disease by controlling BP, cholesterol, smoking and other risk factors, rather than to wait until after a heart attack occurs. We know that this is already occurring. Zheng et al. reported parallel declines in SCD and overall cardiac deaths between 1989 and 1998; the proportion of cardiac deaths that were sudden did not change.5 In the more recent AHA report, SCD declined by 25% from 130.1 per 100,000 in 2000 to 97.1 per 100,000 in 2017 while heart attack deaths fell by 50%.6 We also know that two of the drug classes that have proven effective in the secondary prevention setting—the beta-blockers in post–MI patients and the ACE inhibitors in patients with impaired ventricular function—reduce risk for subsequent SCD. These drugs have been covered in Chapter 11. The present chapter will focus on treatments that are specifically intended to prevent SCD in patients who have suffered a SCA or who are at particularly high risk of SCD due to severe left ventricular dysfunction.7 Specifically, I will review the evidence concerning the use of amiodarone, implantable cardioverter defibrillators, and cardiopulmonary resuscitation.
Amiodarone
After the failure of the sodium channel blockers in the 1989 Cardiac Arrhythmia Suppression Trial (CAST), in which these drugs increased mortality despite suppressing premature ventricular contractions, amiodarone became the drug of choice for treating ventricular arrhythmias.8 Actually, the clinical trial evidence supporting its efficacy in preventing SCA is mixed. A 2004 meta-analysis of 13 small amiodarone trials in patients with acute MI or congestive heart failure showed a significant reduction in SCD.9 Also, in the Optimal Pharmacological Therapy in Cardioverter Defibrillator Patients (OPTIC) trial in patients with an implantable cardioverter defibrillator (ICD), the combination of beta-blocker and amiodarone was far more effective than beta-blockers alone in reducing the frequency of shocks delivered when the ICD detects a potentially life-threatening ventricular arrythmia.10 However, in the NHLBI-sponsored three-armed Sudden Cardiac Death in Heart Failure Trial (SCD-HeFT), mortality in the 845 patients who received amiodarone plus conventional heart failure treatment was not reduced relative to the 847 who received only conventional heart failure therapy.11 The use of amiodarone has declined rapidly in the past decade due to the recognition of a 5% incidence of potentially life-threatening pulmonary toxicity. It has been overtaken by beta-blockers as the first-line drug for patients at high risk for SCD and now ranks only 196th among all drugs with 2.9 million prescriptions in 2017, which represents a 25% drop since 2012.12
Implantable Cardioverter Defibrillators (ICD)
Ultra-high-tech niche devices like ICDs are too labor-intensive and expensive to have had a noticeable impact on national mortality trends but are a godsend for the roughly 60,000 patients who receive them each year.13 The basic idea is for patients who are known to be at very high risk for sudden cardiac arrest (usually because they have already survived a similar episode) to have a device implanted in their chest that senses the onset of a life-threatening ventricular arrhythmia (tachycardia or defibrillation) and automatically delivers an electrical shock that jolts the heart back to a normal rhythm. So each device has internal electrodes to constantly monitor the patient’s electrocardiogram and to deliver a high-voltage shock directly to the heart when needed, a capacity to record and store when and why each shock is delivered, and a lithium battery (implanted under the skin of the chest and replaced every 5–10 years) to provide power. Usually an antiarrhythmic drug (a beta-blocker and/or amiodarone) is given to minimize the number of electrical shocks delivered, which are very unpleasant and disconcerting. Although not all the arrhythmias detected and shocked by an ICD would have otherwise been lethal, the net intended effect is to substantially reduce sudden cardiac deaths and improve survival.
ICDs have been proven more effective in preventing SCD than antiarrhythmic drugs alone in several randomized trials. The 1016-patient NIH-sponsored Antiarrhythmics Versus Implantable Defibrillators (AVID) trial in the U.S., the 659-patient Canadian Implantable Defibrillator Study (CIDS), and the 288-patient Cardiac Arrest Study Hamburg (CASH) trial in Germany each compared ICD placement versus amiodarone and/or metoprolol in resuscitated survivors of sudden cardiac arrest.14 Mortality was reduced in the ICD group relative to antiarrhythmic drugs by 28% in AVID (P=0.02), 20% in CIDS (P=0.14), and 23% in CASH (P=0.08).15 Although only the AVID result surpassed the threshold for statistical significance, the consistency of the three trials is compelling. The 1996 Multicenter Automatic Defibrillator Implantation Trial (MADIT) found an even greater (46%) survival advantage over conventional medical therapy in heart attack survivors with ventricular dysfunction and a documented history of ventricular tachycardia but not SCA.16
Two additional trials in the early years of the 21st century expanded the indications for an ICD beyond patients with known prior episodes of ventricular tachycardia or fibrillation, to all patients with advanced ischemic heart failure. In the MADIT-II trial in 1232 patients with advanced heart failure, mortality was significantly reduced by 69% in the group randomized to receive an ICD versus those randomized to receive only antiarrhythmic drugs.17 In the 3-armed SCD-HeFT, mortality was 23% lower in the 829 patients assigned to receive an ICD than in the 847 patients assigned to receive only conventional heart failure therapy (P=0.007).18 Thus, it seems fair to conclude that ICD placement significantly improves survival by at least 20–30%—perhaps a good deal more—in all patients who are at high risk for sudden cardiac death due to advanced ischemic heart failure and/or a prior life-threatening arrhythmic episode.
Cardiopulmonary Resuscitation (CPR)
The immediate goal of CPR is to quickly establish sufficient cardiac function to sustain a blood pressure that is adequate to perfuse the brain. This is done by using an external defibrillator to administer a high-voltage shock to jolt the heart back to a functional rhythm and by periodically compressing and releasing the chest and inflating and deflating the lungs until a functional spontaneous heartbeat is established. Successfully bringing someone back from the brink of death by CPR is very dramatic—even miraculous—when portrayed on television or in the movies. But the reality is more sobering. Only 10.4% of patients who suffer out-of-hospital SCA survive to hospital discharge, and only 8.2% are discharged without significant neurological impairment.19 And this does not even count many persons who are already dead and cold before a first responder arrives on the scene. To be sure, the 25.9% survival rate for the 18% of patients who have a “shockable” heart rhythm (ventricular tachycardia or fibrillation) when the first responder arrives is far better than the 6% survival rate for the remaining patients who have no electrical activity at all (asystole). Also, survival is far better for patients who have their SCA in a hospital (25.8%) or public place (40%) than for patients having their SCA at home, where they are often unwitnessed by anyone trained in CPR. The hard fact is that anyone who suffers an unwitnessed SCA or in whom more than 10 minutes or so has elapsed before resuscitation is initiated is beyond the reach of CPR.
One does not need a controlled clinical trial to establish that cardiopulmonary resuscitation reduces mortality, since the outcome of sudden cardiac arrest is uniformly fatal without it. However, in the past two decades, there has been intensive research aimed at improving CPR techniques and extending their reach. The NHLBI has been at the center of these efforts. In 2000, the NHLBI initiated a randomized community-based trial called the Public Access Defibrillator (PAD) trial in 993 communities with a combined 19,000+ volunteer responders.20 Lay volunteers were trained in CPR in all 993 communities. Then the communities were randomized to two groups. In one group (496 communities), automated external defibrillators (AED) were placed in public sites like shopping malls, community centers, and apartment complexes. In the control group (497 communities), no AEDs were placed. After four years, there were significantly more survivors of SCA in the AED communities (30 survivors out of 128 SCA) than in the control communities (15 survivors among 107 SCA).
As the PAD trial was winding down, the NHLBI initiated the Home Automated External Defibrillator Trial (HAT) to explore the value of providing 7001 high-risk MI survivors who were not candidates for an ICD with an AED for home use.21 Unfortunately, the group who received a home AED did not show any reduction in mortality. The main reason that the home AED strategy was ineffective is that only 117/160 instances of SCA occurred at home, only 58 of these at-home SCA were witnessed, and the home AED was used in only 32 instances. It would seem that only an ICD can provide useful protection for these patients.
In 2007–15, the NHLBI supported a clinical trial network called the Resuscitation Outcomes Consortium (ROC) which conducted a series of randomized trials designed to optimize resuscitation protocols and techniques.22 Among the issues explored were the optimum ratio of chest compressions to respirations, the use of an impedance device to regulate airflow, and whether it was better to defibrillate 30 seconds or 3 minutes after initiating CPR. These nuances had only a minor impact on SCA survival. The bigger public health issue is how to reach more SCA victims in time, rather than tweaking the process itself.
Impact of Prevention of SCD on Decline in Heart Attack Mortality
In their IMPACT model, Ford et al. attribute 2.5% of the decline in heart attack mortality between 1980 and 2000 to CPR—1.3% for out-of-hospital SCA and 1.2% for in-hospital SCA—and none to amiodarone or ICDs.23 I would quibble with these estimates because the numerators and denominators are mismatched. About half of the SCD prevented by CPR (the numerator) are of non-cardiac etiology (trauma, respiratory failure, etc.) and half the remainder are due to non-atherosclerotic heart disease (cardiomyopathies, genetic conduction disorders, etc.). It is incorrect to represent these prevented SCD as a fraction of the decline in heart attack deaths. Although CPR has improved and reaches more people that it did in 2000, I am skeptical that it accounts for more than 1% of the observed decline in heart attack deaths since 1970. I do agree that amiodarone and ICDs have had a negligible impact on the overall decline in heart attack deaths. Amiodarone usage is declining and has not been proven to actually reduce the incidence of SCD. The impact of ICDs is limited by their rarity—60,000 per year (including replacements). Based on the mortality rate (10% per year) and risk reduction (23%) in SCD-HeFT, ICDs can account for only 1380 SCD prevented annually.24
1. A report from the American Heart Association. AHA Statistical Update: Heart Disease and Stroke Statistics—2020 Update, Chapters 14 and 17. Circulation 2020; 141:e139-e596. OI: 10.1161/CIR.0000000000000757.
Cardiac Arrest Registry to Enhance Survival (CARES) website. https://mycares.net/.
2. RJ Myerburg, J Junttila. Sudden cardiac death caused by coronary heart disease. Circulation 2012; 125:1043–1052.
3. PCSB Protein Data Bank. Molecule of the Month. Sodium Potassium Pump. 2009–2010. https://cbm.msoe.edu/teacherWorkshops/ddtyResources/documents/sodiumPotassiumPump.pdf.
4. CT January, LS Wann, JS Alpert, H Calkins, JE Cigarroa, JC Cleveland, JB Cont, PT Ellinor, MD Ezekowitz, ME Field, KT Murray. 2014 AHA/ACC/HRS Guideline for the Management of Patients with Atrial Fibrillation. A report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines and the Heart Rhythm Society. JACC 2014; 64:2246–2280. Developed in collaboration with the Society of Thoracic Surgeons. http://dx.doi.org/10.1016/j.jacc.2014.03.021.
5. LA Cobb, CE Fahrenbruch, M Olsufka, MK Copass. Changing incidence of out-of-hospital ventricular fibrillation, 1980–2000. JAMA 2002; 288:3008–3013.
6. AHA Statistical Update 2020, Chapters 14 and 17.
U.S. Population Age Profile 1960–97, Centers for Disease Control and Prevention (CDC), National Center of Health Statistics Mortality Data, Table 5: Age-adjusted death rates for selected causes of death by sex, race and Hispanic origin, United States, selected years 1950–2017. https://www.cdc.gov/nchs/hus/contents2018.htm#Table_005.
7. SM Al-Khatib, WG Stevenson, MJ Ackerman, WJ Bryant, DJ Callans, AB Curtis, BJ Deal, T Dickfeld, ME Field, GC Fonarow, AM Gillis, CB Granger, SC Hammill, MA Hlatky, JA Joglar, GN Kay, DD Matlock, RJ Myerburg, RL Page. 2017 AHA/ACC/HRS Guideline for Management of Patients with Ventricular Arrhythmias and the Prevention of Sudden Cardiac Death. A report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Rhythm Society. Circulation 2018; 138:e272-e391. doi: 10.1161/CIR.0000000000000549.
8. Cardiac Arrhythmia Suppression Trial (CAST) Investigators. Preliminary report: effect of encainide and flecainide on mortality in a randomized trial of arrhythmia suppression after myocardial infarction. N Engl J Med 1989; 32:406–12. https://www.ncbi.nlm.nih.gov/pub med/2473403?dopt=Abstract.
9. SJ Connolly. Meta-analysis of anti-arrhythmic drug trials. Am J Cardiol 2004; 84(supplement 1):90–93. DOI: https://doi.org/10.1016/S0002-9149(99)00708-0.
10. SJ Connolly, P Dorian, RS Roberts, M Gent, S Bailin, ES Fain, K Thorpe, J Champagne, M Talajic, B Coutu, GC Cronefield, SH Hohnloser, for the Optimal Pharmacological Therapy in Cardioverter Defibrillator Patients (OPTIC) Investigators. Comparison of beta-blockers, amiodarone plus beta-blockers, or sotalol for prevention of shocks from implantable cardioverter defibrillators. The OPTIC Study: a randomized trial. JAMA 2006; 295:165–171.
11. GH Bardy, KL Lee, DB Mark, JE Poole, DL Packer, R Boineau, M Domanski, C Troutman, J Anderson, SE McNulty, N Clapp-Channing, LD Davidson-Ray, ES Fraulo, DP Fishbein, RM Luceri, JH Ip, for the Sudden Cardiac Death in Heart Failure Trial (SCD-HeFT) Investigators. Amiodarone or an implantable cardioverter-defibrillator for congestive heart failure. N Engl J Med 2005; 352:225–237.
12. RN Fogoros. Amiodarone lung toxicity. verywellhealth. https://www.verywellhealth.com/amiodarone-lung-toxicity-1745988.
ClinCalc DrugStats Database. Amiodarone Hydrochloride. https://clincalc.com/DrugStats/Drugs/AmiodaroneHydrochloride.
13. AHA Statistical Update: Heart Disease and Stroke Statistics—2020 Update, Table 25.2 (2014 data). Circulation 2020; 141:e139-e596. OI: 10.1161/CIR.0000000000000757.
14. The Antiarrhythmics Versus Implantable Defibrillator (AVID) Investigators. A comparison of antiarrhythmic drug therapy with implantable defibrillators in patients resuscitated from near-fatal ventricular arrhythmias. N Engl J Med 1997; 337:1576–1583.
SJ Connolly, M Gent, RS Roberts, P Doran, D Roy, RS Sheldon, LB Mitchell, MS Green, GJ Klein, B O’Brien, for the CIDS Investigators. Canadian Implantable Defibrillator Study (CIDS): A randomized controlled trial of the implantable cardioverter defibrillator against amiodarone. Circulation 2000; 101:1297–1302.
KH Kuck, R Cappato, J Siebels, R Ruppel, for the CASH Investigators. Randomized comparison of antiarrhythmic drug therapy with implantable defibrillators in patients resuscitated from cardiac arrest. Circulation 2000; 102:748–754.
15. RT Borne, D Katz, J Betz, PN Peterson, FA Masouli. Cardioverter-defibrillators for secondary prevention of sudden cardiac death: a review. J Am Heart Assoc 2017; 6:e005515. DOI: 10.1161/JAHA.117.005515.
16. AJ Moss, WJ Hall, DS Cannom, JP Daubert, SL Higgins, H Klein, JH Levine, S Saksena, AL Waldo, D Wilber, MW Brown, M Heo, for the Multicenter Automatic Defibrillator Implantation Trial Investigators. Improved survival with an implanted defibrillator in patients with coronary disease at high risk for ventricular arrhythmia. N Engl J Med 1996; 335:1933–1940.
17. AJ Moss, W Zareba, WJ Hall, H Klein, DJ Wilber, DS Cannom, JP Daubert, SL Higgins, MW Brown, ML Andrews, for the Multicenter Automatic Defibrillator Implantation Trial II Investigators. Prophylactic implantation of a defibrillator in patients with myocardial infarction and reduced ejection fraction. N Engl J Med 2002; 346:877–883.
18. GH Bardy, et al., SCD-HeFT.
19. AHA Statistical Update 2020, Chapters 14 and 17, ibid.
20. The Public Access Defibrillation Trial Investigators. Public-access defibrillation and survival after out-of-hospital cardiac arrest. N Engl J Med 2004; 351:637–646.
21. GH Bardy, KL Lee, DB Mark, JE Poole, WD Toff, AM Tonkin, W Smith, P Dorian, DL Packer, RD White, WT Longstreth, J Anderson, G Johnson, E Bischoff, JJ Yallop, S McNulty, L Davidson, NE Clapp-Channing, Y Rosenberg, EB Schron, for the HAT Investigators. Home use of automated external defibrillators for sudden cardiac arrest. N Engl J Med 2008; 358:1790–1804. DII 10.1056/NEJMoa0801651.
22. RJ Franscone, KG Lurie, JM Goodloe. Resuscitation Outcomes Consortium (ROC) studies dig deep into the science of resuscitation. Journal of Emergency Medical Services 2016, 31 Dec; 42(1). https://www.jems.com/2016/12/31/resuscitation-outcomes-consortium-roc-studies-dig-deep-into-the-science-of-resuscitation/.
23. ES Ford, UA Ajani, JB Croft, JA Critchley, DR Labarth, TE Kottke, WH Giles, S Capewell. Explaining the Decrease in U.S. Deaths from Coronary Disease, 1980–2000. N Engl J Med 2007; 356:2388–2398. DOI: 10.1056/NEJMsa053935.
24. GH Bardy, et al., SCD-HeFT.