4
While simple organisms can get what they need from the environment via simple or assisted diffusion, all higher animals have a circulatory system to deliver oxygen and nutrients to cells that are not in direct contact with the external environment. The circulatory system consists of a vehicle—the blood—to carry oxygen and nutrients to the various organs, a heart to pump the blood, and conduits—the arteries, capillaries, and veins—to carry blood to the organs, perfuse them, and return blood to the heart, respectively. Human beings and other mammals actually have two circulations connected in series—the low-pressure pulmonary circulation, which sends oxygen-depleted blood from the right side of the heart to the lungs and returns oxygenated blood to the left side of the heart, and the high-pressure corporal circulation which send oxygenated blood from the left side of the heart to the rest of the body and returns oxygen-depleted blood to the right side of the heart. The term blood pressure (BP) refers to the force generated by the heart that propels blood from the left ventricle through the arteries in the corporeal circulation. BP is traditionally measured with an inflatable cuff applied to the upper arm and connected to a column of mercury (sphygmomanometer) and a stethoscope to detect changes in the sound of blood flow through the brachial artery in the crook of the elbow. At any given sitting, two pressures are measured—the systolic, when the left ventricle is fully contracted and the pressure is at its peak, and the diastolic, when the left ventricle relaxes and the pressure is at its lowest. In a healthy 35-year-old adult, a pressure sufficient to support a 120-millimeter (mm) column of mercury (Hg) at systole and 80 mm at diastole is typical and is recorded as 120/80 mmHg. The absence of a blood pressure due to massive blood loss and/or a failing heart is incompatible with life.
Blood pressure is not static. It may vary with body position (lying, sitting, or standing), time of day, activity, or state of nervous excitement. Blood pressure normally differs between the arms and legs and may differ between one arm and the other under pathologic conditions like thoracic outlet syndrome. High salt intake can raise blood pressure and may help explain the relatively high prevalence of high blood pressure in traditional Asian cultures. Blood pressure is also regulated by hormones like aldosterone, serotonin, angiotensin, epinephrine (adrenaline), and norepinephrine; derangements in their metabolism by neuroendocrine tumors or kidney failure may raise blood pressure. (The relation of blood pressure and kidney function actually goes both ways; high blood pressure may cause thickening of the kidney arteries and impaired kidney function, while impaired kidney function due to other causes may release angiotensin into the circulation and raise blood pressure.) However, most instances of high blood pressure have no discernable physiologic cause or explanation other than the commonly observed gradual stiffening of arteries with increasing age (arteriosclerosis). This form of hypertension used to be called “idiopathic” or “essential” (meaning that the underlying cause and biological pathways were not understood), but we now recognize that it is largely due to modifiable lifestyle factors, especially diet.
The recognition of high blood pressure (or hypertension) as a condition associated with adverse clinical conditions such as heart failure (subsumed under diseases of the heart), stroke (largely cerebral hemorrhage), and kidney failure—the three leading non-infectious causes of death in 1900—long pre-dates the invention of the sphygmomanometer in 1896.1 Indeed, the recognition of “hard pulse disease” goes back to ancient times. However, the remedies applied over the ages—bloodletting, severe sodium restriction, cutting the sympathetic nerves, and administering pyrogens to cause fever—were neither safe nor effective. Although severe or “malignant” hypertension, defined as a lethal syndrome of extreme rises in BP (e.g., 300 mmHg systolic), retinopathy (arterial changes in the retina that may lead to loss of vision), and kidney failure, leading rapidly to heart failure and/or (usually fatal) bleeding in the brain, was recognized in 1928, the medical establishment remained skeptical about treating lesser elevations in blood pressure. By the 1930s, insurance companies were already well aware of the value of BP in their actuarial calculations.2 Yet in 1937, while President Franklin Roosevelt was suffering from moderate hypertension, eminent American cardiologist Paul Dudley White opined that hypertension was “an important compensatory mechanism that should not be tampered with.”3 Six years earlier, British professor John Hay had gone one step further by opining that “the greatest danger to a man with high blood pressure lies in its discovery, because then some fool is certain to try and reduce it.”4 The question was moot in any case. It was not until after World War II that effective blood pressure-lowering drugs—tetramethylammonium chloride, hydralazine, and reserpine—became available, and it was not until a decade later that the development of the thiazides, well-tolerated oral diuretics derived from the sulfa antibiotics, made the treatment of high blood pressure practical on a mass scale. Other safe and effective drugs—beta- and alpha-adrenergic blockers, calcium channel blockers, angiotensin converting enzyme (ACE) inhibitors, angiotensin receptor blockers (ARB)—would follow in the ensuing two decades.
Although, no systematic surveys of the prevalence of high blood pressure exist before 1950, one can infer from the decline in deaths from associated conditions like stroke (Figure 4.1) and kidney failure, that the prevalence of high blood pressure almost certainly declined between 1900 and 1950, while other cardiovascular risk factors were still on the rise.
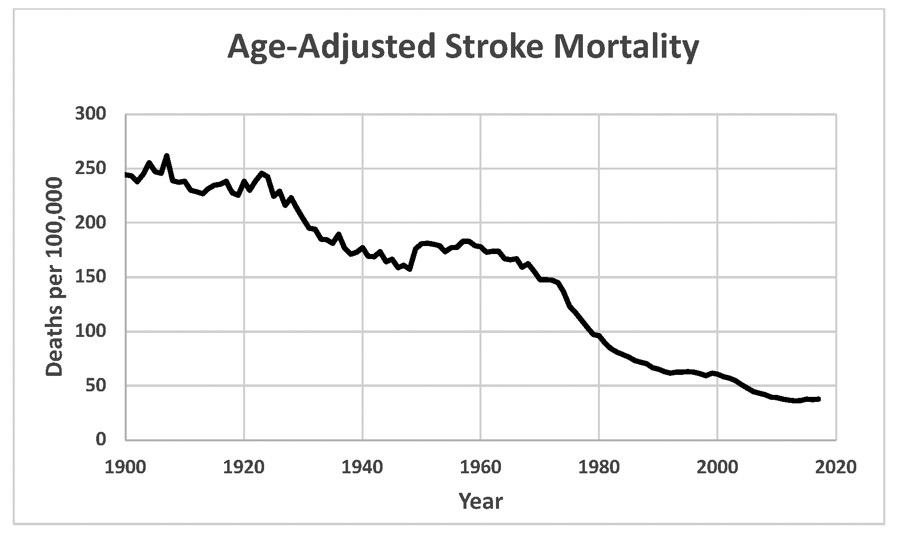
U.S. trend in age-adjusted stroke mortality, 1900–2017. Data were obtained from CDC Vital Statistics compilations.
Now, stroke is complicated, because it reflects a mixture of obstruction of the arteries by ruptured atherosclerotic plaques and thrombosis (clotting) and bleeding in the brain. Today, atherothrombotic strokes are more common, but cerebral bleeds are more lethal. In the early 20th century, cerebral bleeds were both more common and more lethal. The pre–1950 decline in strokes in the face of an increasing trend in atherosclerosis almost certainly reflects a decline in cerebral bleeds and, by inference, hypertension. Since no effective blood pressure treatments existed at that time, this decline may reflect declining salt intake as broad access to refrigeration decreased the reliance on salt to preserve meats. In any case, by the time the Framingham Heart Study began, mortality from strokes (including cerebral bleeds) had already declined by 40% since 1900 and mortality from nephropathy (kidney failure) had declined by 80% (from 88.6 to 17.4 per 100,000).5
When the Framingham Heart Study published its initial follow-up results in the early 1960s, moderate “essential” hypertension (that is moderately elevated BP with no known primary biological cause) was still considered a relatively benign condition.6 According to a prominent 1965 review article, “It is common experience that many patients live medically uneventful lives in spite of prolonged and considerable blood pressure elevation.”7 Of course, a life ending in a sudden fatal heart attack at age 64 was probably considered “medically uneventful” at that time. A common clinical rule of thumb was that a systolic BP below 100 plus the person’s age was considered normal.
Landmark Blood Pressure Trials
Spurred by the early Framingham results and the development of the thiazide diuretics, the U.S. Veterans Administration (VA), a nationwide network of hospitals established to treat military veterans, undertook a groundbreaking randomized clinical hypertension trial.8 The VA Cooperative BP Trial, which began in 1964 under the leadership of Dr. Edward Freis, was the first of many major research trials conducted by the VA and was the among the first trials worldwide to address the treatment of hypertension.9 It had two components:
1. a placebo-controlled trial in 143 male veterans with severe (but not malignant) hypertension (diastolic BP of 115 to 129 mmHg) in which the active treatment group received a combination of hydrochlorothiazide, reserpine, and hydralazine, which lowered their BP by 43/30 mmHg, for a period averaging 1.5 years, and
2. a placebo-controlled trial in 380 male veterans with mild to moderate hypertension (diastolic BP of 90 to 114 mmHg) employing the same three drugs, which lowered their mean diastolic BP by 19 mmHg, for a period averaging 3.8 years.
Although both were very small trials by modern standards and were designed only to detect differences in composite outcomes, including stroke, retinal hemorrhage, heart attack, heart failure, and dissecting aortic aneurysm, as well as mortality, both studies showed that the veterans receiving active drug treatment to lower their blood pressure fared far better than those receiving placebo. In the severe hypertension trial (published in 1967), only one adverse cardiovascular events (no deaths) occurred in the drug-treated patients versus 27 events (including 4 deaths) in the placebo group.10 In the (larger and longer) mild to moderate hypertension trial, which was published in 1970, 22 adverse cardiovascular events (including 8 deaths) occurred in the group receiving active drug treatment versus 56 events (including 19 deaths) in the placebo group.11 Thus, by 1970, the earlier prevailing view that essential hypertension with diastolic BP < 130 mmHg was “benign” had become untenable. By the time I finished medical school in 1973, it was standard practice (at least in theory) to treat all patients with diastolic BP > 90 mmHg, but the goal of attaining diastolic BP below 90 mmHg was seldom attained. The rule of thumb at that time was that only half of all hypertensive patients were diagnosed, only half of those diagnosed were treated, and only half of those treated attained the therapeutic goal of < 90 mmHg diastolic.12 Thus, overall, only one of every eight hypertensive patients was adequately treated.
The VA Cooperative Trial was only the first step. The study was relatively small and did not include women (who comprised only a small fraction of VA patients). Also, the VA trial used a fixed drug regimen, rather than targeting a blood pressure goal. So, in 1971, the NHLBI initiated the Hypertension Detection and Follow-Up Program (HDFP), a non-blinded community-based randomized trial, which used a stepped-care regimen of six blood pressure-lowering drugs in 10,940 men and women, aged 30–69, with diastolic BP > 90 mmHg (average BP = 158/101 mmHg).13 This trial was initiated at NIH by William Friedewald and Gerald Payne, and Herbert Langford, Jeremiah Stamler, Nemat Borhani, and Coordinating Center Director Mort Hawkins were prominent in the study leadership. Patients in the active treatment arm began with a dose of the thiazide-like diuretic (chlorthalidone), and escalating doses of other drugs were added at prespecified intervals according to a standard protocol until the diastolic BP was brought below 90 mmHg. Patients in the control group were referred to outside physicians for standard care (which would presumably reflect the inadequate level of BP control in the community at large). As expected, BP control was significantly better in the stepped care group than in the control group. This difference was enough to bring about a statistically significant (P < 0.01) 17% reduction (6.4 versus 7.7%) reduction in mortality, including a 20% reduction in the milder cases (diastolic BP between 90 and 104 mmHg at baseline).14 Mortality was reduced in both men and women and in both Black and White, and for ages 50–59 and 60–69 years.15 Strokes were also significantly reduced by about one-third (1.9 versus 2.9%) in the stepped care group.16
While skeptics might have dismissed the VA trial results as those of a small trial in an unrepresentative patient population, they could not dismiss the power and generalizability of the HDFP results. Having established the unequivocal value of treating mild to moderate diastolic hypertension, medical scientists around the world began clinical trials to address unanswered questions about how broadly the lessons of these early trials ought to be applied and the role of the many new antihypertensive drugs entering the market as we entered the 1980s. I will focus on a few NHLBI-sponsored clinical trials which were at the center of the U.S. efforts in this arena.
The first question on the post–HDFP agenda was the treatment of systolic hypertension. In the early days, physicians focused on treating elevated diastolic BP, even though systolic BP was the stronger risk factor in the Framingham and other epidemiologic cohort studies. So, even after it was accepted that hypertension, defined by diastolic BP > 90 mmHg, was not a benign disease and that blood pressure lowering drugs could reduce mortality and strokes, questions remained about whether and how to treat the large number of older patients (projected at the time to affect eight million Americans by 2025) whose arteries lost elasticity as they aged and presented with elevated systolic BP (> 160 mmHg) and a normal diastolic BP.17 After all, these were the very sort of patients in whom John Hay and Paul Dudley White had cautioned against medical interference a generation earlier, and their skeptical attitude still prevailed in many quarters. If one were to treat their “isolated systolic hypertension,” would one not risk lowering their diastolic BP to troublesome levels that would produce dizziness, fainting, falls, and even broken bones in fragile seniors? Would lowering BP reduce cardiovascular complications enough to offset these potential risks?
After a successful pilot study led by Steve Hulley and McFate Smith, the NHLBI initiated the Systolic Hypertension in the Elderly Program (SHEP) in 1985 to address this important condition. SHEP was a double-blind placebo-controlled randomized trial in 4736 men and women aged 60 years and above with isolated systolic hypertension (systolic BP > 160 mmHg but diastolic BP < 90 mmHg). The active treatment group received chlorthalidone, supplemented with the beta-blocker atenolol and/or reserpine as needed to lower systolic BP by at least 20 mmHg and to a level below 160 mmHg. The primary outcome of interest was the combined incidence of fatal and nonfatal stroke. The trial was led by many of the same investigators who led the HDFP, but now with Curt Furberg, Jeff Cutler, and Jeff Probstfield leading the NHLBI project team. Once again, the results were resoundingly positive. After an average of 4.5 years of follow-up, a 12 mm Hg reduction the average systolic BP (143 versus 155) was accompanied by a 36% reduction in strokes in the chlortalidone versus the placebo group (5.2% versus 8.2%, P = 0.0003).18 Chlorthalidone treatment also brought about substantial and statistically significant reductions in heart attacks, all major cardiovascular events, and mortality from all causes. The SHEP results confirmed that hypertension, even when confined to elevated systolic BP in older patients with stiff arteries, was a clinically significant condition whose treatment was demonstrably lifesaving.
The next critical question was brought to the fore by the many emerging antihypertensive drug options and the difficulty of attaining adequate BP control with any single drug. The Antihypertensive and Lipid Heart Attack Trial (ALLHAT) was undertaken in 1994 (with a substantial contribution from Pfizer, which provided two of the first-line drugs plus logistical support) to address the question of which drugs, singly or in combination, were best for controlling BP and preventing adverse cardiovascular outcomes.19 ALLHAT was one of the most complex trials the NHLBI has ever undertaken. Not only was it huge—42,448 participants (of whom 47% were women and 53% were non–White)—it included randomization to one of four first-line drugs—lisinopril (an ACE inhibitor), amlodipine (a calcium channel blocker), doxazosin (an alpha-adrenergic blocker), and a low-dose (12.5–25 mg) chlorthalidone (diuretic) control arm.20 Each of these drugs had up to three different prescribed dosage levels which somehow had to be titrated to attain a BP < 140/90 mmHg in each patient (in conformity with the expert guidelines at that time) while maintaining the double-blind design.21 Participants who were unable to attain this goal on the maximum dosage of their first-line drug were also given atenolol (a beta-adrenergic blocker) as a second-line drug; hydralazine, reserpine, and clonidine were used as third-line drugs for patients not controlled on two drugs. Furthermore, to treat and track so many patients, ALLHAT’s 625 clinical sites were distributed into nine administrative regions, each with its own separate leadership structure. And if all that wasn’t enough, one-quarter of the study participants were simultaneously enrolled in a non-blinded pravastatin trial using a partial-factorial design (see Chapter 3). Much of the ALLHAT leadership—Study Chair Curt Furberg (now at Wake Forest Bowman Gray University), Program Director Jeff Cutler, Project Officer Gerald Payne—had been part of the NHLBI leadership team for SHEP, and many of the ALLHAT regional directors and deputy Study Chair Jackson Wright were also SHEP investigators. The Coordinating Center, now led by Barry Davis, remained at the University of Texas at Houston.
The final ALLHAT results showed no significant differences among the four treatment arms in the primary outcome—the combined incidence of fatal and non-fatal heart attacks—or in most of the secondary cardiovascular outcomes and total mortality.22 The exception was a significantly lower rate of heart failure diagnoses and hospitalizations in the chlorthalidone control group and significantly higher rates of heart failure in the doxazosin group.23 (The latter finding, along with its lower efficacy in achieving BP control, caused the doxazosin arm to be terminated early.) It should be noted that the clinical significance of the ALLHAT heart failure results is uncertain because diuretics tend to alleviate heart failure by decreasing fluid retention, while doxazosin tends to increase fluid retention. At the time, the ALLHAT results were touted because they showed that the least expensive drug (chlorthalidone) was as good or better than the newer more expensive drugs. But even now, almost two decades later, when inexpensive generic versions of all these drug classes are available, ALLHAT was useful in establishing the therapeutic equivalence of these drug classes, which are now often used in combination, since one drug is rarely sufficient to achieve optimal BP control.
The final major remaining question in treating hypertension was how low is low enough. Two non-blinded 21st-century randomized trials set out to determine whether cardiovascular outcomes might be further improved by lowering the goal for systolic BP from < 140 mmHg (“standard control”) to < 120 mmHg (“intensive control”). The first trial, initiated by Peter Savage and Jeff Cutler, was conducted in 2001–09 in a 4733-participant subset of a type 2 diabetes trial called Action to Control Cardiovascular Risk in Diabetes (ACCORD), which employed a partial factorial design (see Chapter 3).24 The second, the Systolic Blood Pressure Intervention Trial (SPRINT), was initiated by Jeff Cutler and project officer Larry Fine and conducted in 2010–15 in 9361 non-diabetic patients.25 Both trials achieved substantially lower SBP in the intensive than in the standard control groups,. SPRINT found a statistically significant 25% reduction in the primary composite cardiovascular outcome and a significant 27% reduction in total mortality in non-diabetic patients randomized to intensive versus standard control.26 However, the ACCORD trial found only a small (12%) non-significant reduction in cardiovascular events in diabetic patients randomized to the intensive versus standard treatment group.27 At first glance, these two trials appeared to show better results for intensive BP control in non-diabetic than diabetic hypertensive patients. However, a subsequent analysis of the ACCORD BP trial showed that the benefit of intensive BP control in ACCORD participants who were randomized to standard glycemic control—a 23% reduction in cardiovascular events—was essentially identical to the 25% reduction in SPRINT.28 This squares with a subgroup analysis of the SHEP trial, in which lowering systolic BP to 140 mmHg or less significantly reduced adverse cardiovascular outcomes in older diabetic, as well as non-diabetic participants.29 It was only the ACCORD patients who were randomized to the failed intensive glycemic control strategy who did not benefit from the intensification of BP control. It should also be noted that the improved cardiovascular outcomes in the intensive BP treatment groups in both the SPRINT and ACCORD trials came at the cost of statistically significant increases in complications related to low BP—dizziness, fainting, injuries sustained in falls, etc., although the benefits clearly outweighed the risks. The 2017 ACC/AHA High Blood Pressure Clinical Practice Guidelines revised the threshold and treatment goal for hypertension to 130/70 mmHg, reflecting the SPRINT results.30
Quantitative Overview of BP Trials
The studies I have highlighted in this chapter represent only major landmark trials, which were sponsored mainly in the U.S. public sector, although sometimes (especially in ALLHAT) with significant participation from non–U.S. sites and in-kind contributions from pharmaceutical firms. The reason for the preeminence of NIH, the world’s largest public funding source for biomedical research, in the blood pressure field is that trials of stepped care approaches to BP control using combinations of drug classes and trials of head-to-head drug comparisons are generally not in the wheelhouse of drug manufacturers, who as a rule are interested in proving the efficacy of their specific drug. (As we shall see in Chapter 5, the pharmaceutical industry has played a far more prominent role in cholesterol trials.) However, these large NIH trials are but the tip of the iceberg of BP trials conducted in the U.S. and throughout the world.31 A 2016 retrospective meta-analysis, found 123 qualifying BP trials, including 613,815 participants.32 Notwithstanding the many pitfalls of retrospective meta-analysis (see Chapter 3), these investigators were quite meticulous and transparent about their eligibility criteria. Also, by 2016, the overall benefit of the BP treatment was no longer controversial; the authors’ intent was simply to quantify the relationship between BP lowering and various cardiovascular outcomes is specific subgroups. Their main findings were as follows:
1. The risk of major adverse cardiovascular outcomes fell by 20% (strongly significant) for every 10 mmHg reduction in systolic BP. This is actually larger than the 12% decrease in 10-year risk associated in observational studies with a 10 mmHg drop in systolic BP in a 60 year-old White male non-smoker without diabetes.33
2. Every 10 mmHg in systolic BP was also associated with a 17% decrease in risk of heart attack, a 27% decrease in risk of stroke, a 28% decrease in risk of heart failure, and a 13% decrease in mortality—all strongly significant.
3. Similar benefits of BP lowering at all baseline levels of BP.
4. Similar benefits of BP lowering in patients with and without cardiovascular disease at baseline.
5. Similar benefits of BP lowering for most classes of drugs, with the exception of beta-blockers (which were significantly less effective than other drug classes with respect to all outcomes except heart attack).
Impact of BP Control on Decline in Heart Attack Deaths
In a span of 60 years, the treatment of hypertension has traveled a long road from therapeutic nihilism, with no effective treatments available anyway, to a clear mandate for lowering BP below 130/80 mmHg, with a wide variety of safe and effective drugs to accomplish this goal in most patients. Indeed, four of these drugs—lisinopril, amlodipine, losartan, and hydrochlorothiazide are—ranked first, fifth, ninth, and twelfth among the most frequently prescribed drugs in the U.S. in 2017 with more than 270 million prescriptions among them.34
Clearly, our progress in developing blood pressure drugs and demonstrating their efficacy has profoundly affected clinical practice, expanding the definition of hypertension and increasing the proportion of hypertensives successfully treated. A recent analysis of data from the National Health and Nutrition Examination Survey (NHANES) documents this progress.35 In the 1999–2000 survey, 31.8% of persons with hypertension were treated and controlled to BP <140/90 mmHg. By 2013–14 this percentage had climbed to 53.8%. However, this percentage has tailed off to 48.4% in 2015–16 and 43.7% in 2017–18. This unfortunate trend probably reflects the relaxation of the systolic BP treatment goal from < 140 to < 150 mmHg in the eighth Joint National Committee (JNC 8) treatment guidelines in 2014.36 It remains to be seen whether the incorporation of the SPRINT results in the newest national guidelines, issued in 2018, will reverse that trend.37
To what extent do these trends explain the observed decline in mortality from heart attacks and strokes? Ford et al. have used a sophisticated model called IMPACT to address this question for coronary disease (heart attack) mortality in the U.S. for the 20-year period 1980–2000, during which heart attack mortality declined by 45.9% from 345.2 to 186.8 deaths per 100,000.38 This model, which I will be citing throughout this book, analyzes prevalence and mortality rates, broken down into specific categories by age and gender, and applies regression coefficients estimated from the best available observational data for BP and other risk factors. It estimates that the change in mean systolic BP from 129.0 to 123.9 mmHg would be expected to have prevented 68,000 heart attack deaths in 2000—about 20.1% of the observed reduction in heart attack mortality.
The obvious problem with the IMPACT model is that it does not consider advances in BP treatment or declines in heart attack mortality after 2000, when heart attack mortality declined at its fastest pace (see Figure 1.2) and the proportion of hypertensive patients who attain a BP < 140/90 mmHg nearly doubled. Lacking access to the IMPACT software and the required input data, I have devised a method to update the published 1980–2000 result to 2014 using the NHANES reports cited above (see the appendix for details). Applying the fact that the improvement in BP control from essentially zero in 1968 to 53.8% in 2014 is 2.47 times the improvement from 10% in 1980 to 31.8% in 2000, we calculate that BP lowering accounted for 26.7% of the 79.5% decline in heart attack mortality during that period (see Table A.2).39 This figure understates the total cardiovascular benefit of BP control, since it does not include the considerable impact of BP control on strokes and heart failure. However, this estimate would drop to 22% if we used the 2017–18 NHANES BP control figure. In either case, our advances in the treatment and control of high blood pressure since 1960 are a major success story and have taken a big bite out of the mid–20th-century cardiovascular pandemic.
1. Wikipedia. History of Hypertension. https://en.wikipedia.org/wiki/History_of_hypertension. MG Sakayan, NV Deshpanda. Timeline of history of hypertension treatment. Front Cardiovasc Med 2016; 33:1–14, doi: 10.3389/fcvm.2016.00003, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4763852.
2. TA Kotchen. Historical trends and milestones in hypertension research. A model of the process of translational research. Hypertension 2011; 58:522–538.
3. PD White. Heart Disease. New York: Macmillan, 2nd edition, 1937, p. 326.
4. J Hay. A British Medical Association Lecture on the Significance of a Raised Blood Pressure. British Medical J July 11, 1931; 2 (3679): 43–47.
5. Morbidity and Mortality. 2012 Chartbook on Cardiovascular, Lung and Blood Diseases, NIH-NHLBI. Chart 3–24. https://www.nhlbi.nih.gov/files/docs/research/2012_ChartBook_508.pdf.
Centers for Disease Control. Age-adjusted death rates for 69 selected causes by race and sex using year 2000 standard population: United States, 1950–59. https://www.cdc.gov/nchs/data/dvs/hist293_1950_59.pdf, 1960–67. https://www.cdc.gov/nchs/data/mortab/aadr6067.pdf, 1968–78. https://www.cdc.gov/nchs/data/mortab/aadr6878.pdf.
Centers for Disease Control and Prevention (CDC), National Center of Health Statistics. Mortality Data Finder. Table 5: Age-adjusted death rates for selected causes of death by sex, race and Hispanic origin: United States, selected years 1950–2017, https://www.cdc.gov/nchs/hus/contents2018.htm#Table_005 (Excel spreadsheet link).
6. M Moser. Historical perspective on management of hypertension. J Clin Hypertens 2006; 8:15–20. https://online library.wiley.com/doi/full/10.1111/j.1524-6175.2006.05836.x.
7. W Goldring, H Chasis. Antihypertensive drug therapy: an appraisal. Arch Intern Med 1965; 115:523–25.
8. U.S. National Library of Medicine. The VA Cooperative Study and the Beginning of Routine Hypertension Screening, 1864–1980. The Edward D. Freis Papers. https://profiles.nlm.nih.gov/spotlight/xf/feature/study.
9. J Cutler, SW MacMahon, CD Furberg. Controlled clinical trials of drug treatment for hypertension: A review. Hypertension 1989; 13(suppl I):I36-I44.
10. Veterans Administration Cooperative Study Group on Anti-Hypertensive Agents. Effects of treatment on morbidity in hypertension. Results in patients with diastolic blood pressures averaging 115–129 mm Hg. JAMA 1967; 202:1028–34.
11. Veterans Administration Cooperative Study Group on Anti-Hypertensive Agents. Effects of treatment on morbidity in hypertension. II Results in patients with diastolic blood pressure averaging 90–114 mm Hg. JAMA 1970; 213:1143–52.
12. VL Burt, JA Cutler, M Higgins, MJ Horan, D Labarth, P Whelton, C Brown, EJ Rocella. Trends in the prevalence, awareness, treatment, and control of hypertension in the adults U.S. population. Data from the Health Examination Surveys, 1960 to 1991. Hypertension 1995; 26:1–60, https://www.ahajournals.org/doi/epub/10.1161/01.HYP.26.1.60.
13. ClinicalTrials.gov. The Hypertension Detection and Follow-Up Study (HDFP). https://clinicaltrials.gov/ct2/show/NCT00000485?term=HDFP&draw=2&rank=1.
14. Hypertension Detection and Follow-Up Program Cooperative Group. Five Year Findings of the Hypertension Detection and Follow-Up Program. I. Reduction in mortality of persons with high blood pressure, including mild hypertension. JAMA 1979; 242:2562–71.
15. Hypertension Detection and Follow-Up Program Cooperative Group. Five Year Findings of the Hypertension Detection and Follow-Up Program. II. Mortality by age, race, and sex. JAMA 1979; 242:2572–77.
16. Hypertension Detection and Follow-Up Program Cooperative Group. Five Year Findings of the Hypertension Detection and Follow-Up Program. III. Reduction in stroke incidence among persons with high blood pressure. JAMA 1982; 247:633–638.
17. NO Borhani, WB Applegate, JA Cutler, BR Davis, CD Furberg, E Lakatos, L Page, M Perry, WM Smith, JL Probstfield. Part 1: Rationale and Design. Hypertension 1991; 17(suppl II):1–15.
ClinicalTrials.gov. Systolic Hypertension in the Elderly Program (SHEP). https://clinicaltrials.gov/ct2/show/record/NCT00000514?term=SHEP&draw=2&rank=4.
18. SHEP Cooperative Research Group. Prevention of stroke by antihypertensive drug treatment in older persons with isolated systolic hypertension. Final results of the Systolic Hypertension in the Elderly Program (SHEP). JAMA 1991; 265:3255–64.
19. The Antihypertensive and Lipid Heart Attack Trial (ALLHAT) ClinicalTrials.gov. https://clinicaltrials.gov/ct2/show/record/NCT00000542?term=ALLHAT&draw=2&rank=3.
20. RH Grimm, KL Margolis, V Papademetriou, WC Cushman, CE Ford, J Bettencourt, MH Alderman, JN Basile, HR Black, V DeQuattro, J Eckfeldt, CM Hawkins, HM Perry, M Proschan. Baseline characteristics of participants in the Antihypertensive and Lipid Heart Attack Trial (ALLHAT). Hypertension 2001; 37:19–27.
21. The sixth report of the Joint National Committee on prevention, detection, evaluation, and treatment of high blood pressure. Arch Intern Med 1997; 157:2413–2446.
22. The Antihypertensive and Lipid Lowering Treatment to Prevent Heart Attack Trial (ALLHAT). JAMA 2000; 283:1967–1975. The Antihypertensive and Lipid Heart Attack Trial (ALLHAT) Research Group. Major outcomes in high-risk hypertensive patients randomized to angiotensin-converting enzyme inhibitor or calcium channel blocker vs diuretic. JAMA 2002; 288:2981–2997.
23. The ALLHAT Officers and Coordinators for the ALLHAT Collaborative Research Group. Major cardiovascular events in hypertensive patients randomized to doxazosin vs chlorthalidone: the Antihypertensive and Lipid-Lowering Treatment to Prevent Heart Attack Trial (ALLHAT). JAMA 2000; 283:1967–1975.
24. ClinicalTrials.gov. Action to Control Cardiovascular Risk in Diabetes (ACCORD). https://clinicaltrials.gov/ct2/show/NCT00000620?term=accord&draw=2&rank=1.
25. ClinicalTrials.gov. Systolic Blood Pressure Intervention Trial (SPRINT). https://clinicaltrials.gov/ct2/show/record/NCT01206062?term=sprint&cond=High+Blood+Pressure&draw=2&rank=4.
26. The SPRINT Research Group. A randomized trial of intensive versus standard blood pressure control. N Engl J Med 2015; 373:2103–2116.
27. The ACCORD Study Group. Effects of intensive blood-pressure control in type 2 diabetes mellitus. N Engl J Med 2010; 362:1575–1585.
28. S Beddhu, GM Chertow, T Greene, PK Whelton, WT Ambrosius, AK Cheung, J Cutler, L Fine, R Boucher, G Wei, C Zhang, H Kramer, AP Bress, PL Kimmel, S Oparil, CE Lewis, M Rahman, WC Cushman. Effects of intensive systolic blood pressure lowering on cardiovascular events and mortality in patients with type 2 diabetes mellitus on standard glycemic control and in those without diabetes mellitus: Reconciling results from ACCORD BP and SPRINT. J Am Heart Assoc 2018; 7(18):1–14. doi: 10.1161/JAHA.118.009326.
29. JD Curb, SL Pressel, JA Cutler, PJ Savage, WB Applegate, H Black, G Carmel, BR Davis, PH Frost, N Gonzalez, G Guthrie, A Oberman, GH Rutan, J Stamler, for the Systolic Hypertension in the Elderly Program Cooperative Research Group. Effect of diuretic-based antihypertensive treatment on cardiovascular disease risk in older diabetic patients with isolated systolic hypertension. JAMA 1996; 276:1896–1892.
30. PK Whelton, RM Carey, WS Aronow, DE Casey, KJ Collins, CD Himmelfarb, SM DePalma, S Goldring, KA Jamerson, DW Jones, EJ MasLaughlin, P Munter, B Ovbiagele, SC Smith, CC Spencer, RS Stafford, SJ Taler, RJ Thomas, KA Williams, JD Williamson, JT Wright. 2017 ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/PCNA Guideline for the Prevention, Detection, Evaluation, and Management of High Blood Pressure in Adults: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Circulation 2018; 138:e484-e594. DOI: 10.1161/CIR.0000000000000596. https://www.ahajournals.org/doi/pdf/10.1161/CIR.0000000000000596.
31. MA Pfeffer, JJV McMurray. Lessons in uncertainty and humility—clinical trials involving hypertension. N Engl J Med 2016; 375:1756–1766. DOI: 10:1056/NEJMra1510067.
32. D Ettehad, CA Emdin, A Kiran, SG Anderson, T Callender, J Emberson, J Chalmers, A Rodgers, K Rahimi. Blood pressure lowering for prevention of cardiovascular disease and death: a systematic review and meta-analysis. Lancet 2016; 387;957–967.
33. AHA/ACC Heart Risk Calculator, http://www.cvriskcalculator.com/.
34. ClinCalc DrugStats Database. The top 200 drugs of 2020. https://clincalc.com/DrugStats/Top200Drugs.aspx.
35. P Muntner, ST Hardy, LJ Fine, BC Jaeger, G Wozniak, EB Levitan, LD Colantonio. Trends in blood pressure control among U.S. adults with hypertension, 1999–2000 to 2017–2018. JAMA 2020; doi:10.1001/jama.2020.14545.
36. PA James, S Oparil, BL Carter, WC Cushman, D Dennison-Himmelfarb, J Handler, DT Lackland, ML LeFevre, TD MacKenzie, O Ogedegbe, SC Smith, LP Svetky, SJ Taler, RR Townsend, JT Wright, AS Narva, E Ortiz. Evidence-based guideline for the management of high blood pressure in adults: report from the panel members appointed to the Eighth Joint National Committee (JNC 8). JAMA 2014; 311(5):507–520. doi:10.1001/jama.2013.284427.
37. PK Whelton, et al.
38. ES Ford, UA Ajani, JB Croft, JA Critchley, DR Labarth, TE Kottke, WH Giles, S Capewell. Explaining the Decrease in U.S. Deaths from Coronary Disease, 1980–2000. N Engl J Med 2007; 356:2388–2398. DOI: 10.1056/NEJMsa053935.
39. VL Burt, et al., Munter, et al.