7
After reading the last three chapters, which attribute more than half of the decline in heart attack deaths since 1960 to improvements in just three risk factors—BP, LDL cholesterol, and smoking—a reader might form the mistaken impression that taming this great pandemic was a direct march from one success to the next. However, the next three chapters, in which promising beginnings have ended in disappointment, offer a sobering look at how difficult and frustrating this process has often been.
Diabetes mellitus (a composite of the Greek word diabainein meaning “to pass through,” referring to excessive urination, and the Latin word mellitus, meaning “sweetened with honey,” referring to the spillage of the sugar glucose into the urine) is a complex metabolic disorder characterized by the inability to regulate blood sugar levels. The underlying defect in this disease, which affects 34.2 million Americans (10.5% of the U.S. population), is a deficiency of or resistance to the hormone insulin, which is normally synthesized in the pancreas by the islets of Langerhans.1 This hormone, which is a dipeptide (two linked chains of amino acids that are shorter than proteins), is integral to the conversion of fat to glucose and enables glucose to enter muscle and other cells to be utilized as an energy source. Diabetes mellitus is actually two distinct diseases—one in which insulin is not produced (type 1) and another in which insulin is produced normally but the target cells are resistant (type 2).
Type 1 diabetes, which typically strikes in children and young adults and is often called juvenile-onset diabetes, has been around for at least 3000 years, since the days of ancient Egypt.2 It is now widely seen as an auto-immune disease, in which the insulin-producing cells of the pancreas are destroyed by the body’s own immune cells, perhaps triggered by a viral infection.3 Without insulin, the constant loss of glucose in the urine produces dehydration, emaciation, and eventually a lethal condition called diabetic ketoacidosis in which blood glucose levels skyrocket and form ketones, the blood becomes more acidic, and coma and death ensue. Until Frederick Banting, James MacLeod, Charles Best, and James Collip, of the University of Toronto isolated insulin in a stable injectable form in the early 1920s—a discovery that won Banting and MacLeod the 1923 Nobel Prize in Medicine—most diabetics succumbed to this fate.4 When Ely Lilly and Company began to mass-produce insulin from the pancreases of pigs and cows in 1923, diabetics gained a new lease on life. However, as diabetics began to live longer, the long-term chronic inflammatory effects of this disease on blood vessels became manifest.5 Two kinds of blood vessel changes occur:
• Changes in the small vessels (microvascular disease) of the heart, kidneys, retina (eyes), nervous system, etc., which may lead to heart failure, kidney failure, blindness, neuropathy, and poor wound healing.
• Accelerated atherosclerosis of large blood vessels (macrovascular disease) in the heart, brain, etc.
Today, the leading cause of death among diabetes is not diabetic ketoacidosis but heart attack, as illustrated by the death of baseball Hall of Famer Jackie Robinson.6 The availability of insulin saved him from an early death by ketoacidosis and allowed him to finish his baseball career, but it did not save him from near-blindness and a fatal heart attack on October 24, 1972.
After World War II, accompanying the post-war boom in prosperity, a once uncommon variant of diabetes called type 2 (or sometimes adult-onset or non-insulin-dependent) diabetes has emerged and has far surpassed type 1 diabetes in prevalence, accounting for 90–95% of all cases.7 In contrast to type 1 diabetes, the pancreas produces more than enough insulin, but the target muscle and fat cells become resistant to insulin and require ever-increasing insulin levels to properly metabolize glucose.8 Unlike the type 1 variant, type 2 diabetes is associated with obesity and manifests as a continuum from “metabolic syndrome” to “pre-diabetes” to frank diabetes. It often evolves slowly over many years (hence, its relative rarity in children). Blood glucose levels rarely rise as high in type 2 as in type 1 diabetes, and ketoacidosis is rare, occurring only in late cases after the ability of the pancreas to meet the ever-increasing demand for insulin has been exhausted. Many type 2 diabetic patients do not require insulin injections and can be adequately controlled by diet, alone or in combination with the myriad available oral agents that stimulate pancreatic insulin production or decrease insulin resistance. However, notwithstanding all these differences, the impact of type 2 diabetes on small blood vessels in the heart, kidneys, eyes, and nervous system is similar to that seen in type 1 diabetes. Like Jackie Robinson and his fellow type 1 diabetics, most type 2 diabetics eventually die of heart attacks, at a rate three times higher than persons without diabetes.
With diabetic ketoacidosis becoming less of an issue following the introduction of insulin and the rise of the type 2 form of the disease, the attention of medical science has focused on how to prevent or ameliorate the cardiovascular consequences of diabetes that shorten the lives of those afflicted and impair the quality of their lives. Since the early 1970s, improving blood glucose control has seemed the most likely avenue to improve the longevity and quality of life in diabetes. Two developments made it possible to pursue this research.
1. Discovery of a superior marker of metabolic control in diabetes: Measuring blood glucose itself is an unsatisfactory marker of metabolic control, since its levels fluctuate widely over the course of each day, depending on how recently one has eaten and the content of the most recent meal. When I was in medical school, the cumbersome glucose tolerance test, which required a series of timed blood draws following ingestion of a measured glucose load, was typically used to diagnose diabetes. The discovery and development of glycated hemoglobin (HbA1c) in the early 1970s provided an easily measured blood marker of metabolic control for tracking the progress of diabetics without worrying about transitory fluctuations in blood glucose levels.9 Selvyn et al. showed in 2010 that HbA1c was indeed a better predictor of future cardiovascular events in 11,092 nondiabetic adults than fasting blood glucose.10 HbA1c levels below 5.7% are generally considered normal, levels between 5.7 and 6.4% indicate prediabetes, and confirmed levels of 6.5% or higher indicate diabetes.11 In diabetics, where HbA1c levels may exceed 10% before treatment, the American Diabetes Association (ADA) considers HbA1c levels below 7% as the criterion for good metabolic control.12
2. Development of a wide variety of oral medications for treating type 2 diabetes.13 Until the late 1990s, therapeutic options for diabetes beyond insulin injection were limited to the biguanides (mainly metformin), the sulfonylureas (glyburide, glipizide, glimepiride), and the meglitinides (repaglinide, nateglinide). Metformin, which improves sensitivity to insulin, is generally considered the drug of choice.14 It is currently the fourth most prescribed drug in the U.S., with 78,602,870 prescriptions written in 2017.15 The less preferred sulfonylureas and meglitinides stimulate pancreatic insulin secretion and are often prescribed in combination with metformin. Many other options have become available during the past two decades, as you will see later in this chapter.
Numerous randomized trials using one or more oral drugs instead of or in addition to insulin have been performed to try to establish, analogous to the blood pressure trials described in Chapter 4, that achieving tighter glucose control in diabetic patients reduces their rate of heart attacks and other adverse cardiovascular events and to determine which if any regimens are most effective in this regard. The major diabetes trials are described below.
University Group Diabetes Program (UGDP)
Diabetes trials got off to a very inauspicious beginning when the UGDP trial was launched in 1960. The trial was originally designed with four treatment arms:
• Tolbutamide (an early sulfonylurea drug that is no longer used)
• Placebo for tolbutamide
• Insulin provided in a standard invariant dosage, set according to the patient’s body weight
• Insulin provided in variable dosages designed to normalize fasting blood glucose levels
In 1961, two more treatment arms were added:
• Phenformin (which has been replaced by metformin in current practice)
• Placebo for phenformin
The study was partially blinded; patients knew whether they were receiving insulin or either of the two oral drugs but did not know whether they received the active or placebo versions of the two oral drugs. The tolbutamide arm was stopped in 1969 because of excess mortality in the group receiving active versus placebo tolbutamide, although the heart attack rates did not differ significantly. The phenformin arm was terminated for lack of efficacy two years later.16 The insulin arms of the trial were allowed to run to completion, but at the end of the day, they were also no better than placebo in terms of preventing heart attacks or prolonging life. The decision by the investigators to abort the tolbutamide arm, which was leaked to the press three weeks before the results were presented at the annual ADA scientific meeting and caused stock prices to plunge, set off a firestorm of criticism, particularly in the pharmaceutical sector, which accused the investigators of bias.17 However, subsequent laboratory studies have shown that tolbutamide (along with a related subset of sulfonylurea drugs) had specific toxic effects on heart muscle that may have accounted for the excess deaths. These drugs have given way to new safer sulfonylurea drugs. Phenformin has since been withdrawn because of its tendency to cause severe lactic acidosis, a metabolic complication that can cause kidney failure and sometimes death.18 Metformin, which is far safer than phenformin, is currently the only approved biguanide drug, So the controversy about the two UGDP oral drugs has been rendered moot to some extent. Yet, the fact remains that it failed to offer “proof of concept” for the hypothesis that improved metabolic control prevents or ameliorates the cardiovascular consequences of diabetes. There things languished for more than a decade.
The Diabetes Control and Complications Trial (DCCT)
In 1983, the NIH’s National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK) launched a major randomized cardiovascular outcomes trial in 1441 patients, aged 13–39 years, with type 1 diabetes mellitus. Patients were stratified (as primary or secondary) based on the absence or presence of pre-existing diabetic complications in the small blood vessels of the eyes and/or kidneys and randomized to conventional or intensive therapy. Patients in the conventional therapy arm received one or two daily injections of a fixed insulin dosage, while patients in the intensive therapy arm received multiple daily doses of insulin with a goal of achieving normal HbA1c levels. The results were published in 1993.19 Mean HbA1c levels of 7% were in fact sustained in the intensive group versus 8.5–9.2% in the conventional group. This difference in glycemic control brought about highly significant reductions in retinopathy (damage to the small blood vessels in the eyes) and other forms of diabetic damage to the microvasculature of the nervous system from close to 60% in the conventional arm to 25% or less in the intensive arm. Reduced rates of other microvascular complications were also observed. However, the DCCT was unable to address the impact of the intensive treatment regimen on incidence of heart attack, stroke, and other macrovascular adverse outcomes, since participants were too young to be at high risk for these outcomes. Two small contemporaneous trials in Stockholm and Japan found similar results.20
UK Prospective Diabetes Study (UKPDS)
The UKPDS was a large complex non-blinded British multicenter randomized trial conducted in 4075 patients with newly diagnosed type 2 diabetes.21 Its objective was to determine wither intensive diabetes control (target HbA1c < 7%) could reduce the incidence of microvascular and macrovascular complications of diabetes. The UKPDS stratified patients as overweight (N = 1704) or normal weight when they entered the study. Normal-weight patients were randomized to receive intensive care with either insulin or a selection of sulfonylurea drugs versus conventional care.22 Overweight patients were randomized to intensive care with either insulin, a sulfonylurea, or metformin versus conventional care.23 Thus, there were in effect seven treatment arms—5 receiving intensive treatment with either insulin, sulfonylureas, or metformin and two receiving conventional care. However, the metformin group was very small (N = 342). The results, published in 1998, were correspondingly complicated, but boiled down to the following:
• Intensive treatment in general significantly reduced microvascular complications.
• Heart attack rates were also reduced in the intensive care groups, but the reduction fell short of statistical significance.
• Intensive treatment had no impact on mortality.
• The intensive treatment metformin group appeared to fare slightly better than the other intensive treatment regimens in overweight patients, but the numbers were small, and the differences were not significant.
In general, the UKPDS results were far more encouraging than the UGDP. The good news is that they showed that intensive glycemic control mitigated the microvascular ravages of type 2 diabetes. The bad news is that they fell well short of proving that this treatment prevented heart attacks. The worse news is that they provided no evidence at all that intensive glycemic control prolonged life. However, the positive results for microvascular complications elevated the HbA1c < 7.0% treatment goal to standard practice and thereby made it mandatory that this treatment goal be incorporated in the control arm of any future diabetes treatment trial. Thus, as the new millennium dawned, it was no longer possible to design an ethically acceptable randomized trial to prove that attaining that goal reduced mortality.
Diabetes trials in the first decade of the 21st century focused chiefly on two research questions: (1) trials comparing a new class of drugs, the thiazolidinediones, to the older drugs (insulin, metformin, and the sulfonylureas) in type 2 diabetes and (2) trials designed to compare even more intensive regimens of glycemic control to the new standard of HbA1c < 7.0%.
The Thiazolidinediones
From the time of the UGDP through the completion of the UKPDS, the medical management of type 2 diabetes relied on same four drug classes—insulin, biguanidines, sulfonylureas, and meglinitides. While phenformin gave way to metformin, tolbutamide gave way to glyburide, glipizide, and glimepiride, and insulin became available in multiple long-acting and short acting variations, the approval of the first thiazolidinedione, troglitazone, in 1997 appeared to represent a breakthrough. Like metformin, troglitazone addressed the basic metabolic defect of type 2 diabetes, by decreasing resistance to insulin. Unfortunately, troglitazone was withdrawn in 2000 because of case reports of significant toxicity to the liver. However, two other drugs of the same class but without the liver toxicity—rosiglitazone and pioglitazone—quickly filled the breech.
Several major cardiovascular trials were soon implemented to test whether these new drugs offered any advantage over the established drugs in reducing cardiovascular complications in diabetes:
1. The Rosiglitazone Evaluated for Cardiac Outcomes and Regulation of Glycaemia in Diabetes (RECORD) trial was a multicenter, randomized, non-blinded study, sponsored by SmithKlineGlaxo, that evaluated the incremental effect of rosiglitazone (Avandia) on cardiovascular outcomes in 4447 patients with type 2 diabetes treated with metformin or sulfonylurea.24
2. The NIH-sponsored Bypass Angioplasty Revascularization Investigation 2 Diabetes (BARI-2D) trial (for which I was the initial project officer) was a 2×2 factorial trial in type 2 diabetic patients with heart disease who were candidates for elective coronary bypass surgery or placement of coronary stents.25 In the diabetes component of the trial, participants were randomized to an “insulin-sensitizing strategy” of glycemic management built around rosiglitazone and metformin versus an “insulin-providing” strategy built around sulfonylureas and insulin. The HbA1c target was < 7.0% in both groups.
3. The PROactive (PROspective pioglitzAzone Clinical Trial In macrovascular Events) study was a multicenter randomized placebo-controlled trial sponsored by Takeda to evaluate the incremental effect of piaglitazone (Actos) above metformin and sulfonylureas on cardiovascular outcomes in 5238 patients with type 2 diabetes and pre-existing cardiovascular disease.26
None of the three trials showed significant improvements in their primary outcomes, although PROactive came close and did achieve a significant reduction in its major secondary outcome, the composite of all-cause mortality, and nonfatal heart attack. However, both rosiglitazone and pioglitazone have since been shown to be associated with significant excess risk of heart failure. This side-effect has relegated these drugs to second-line status in treating diabetes; they are not recommended for patients with known heart failure or significant heart disease.27
Intensification of Diabetes Control
At the outset of the 21st century, four randomized trials were implemented to evaluate the effect of more ambitious HbA1c targets on cardiovascular outcomes:
• The Action to Control Cardiovascular Risk in Diabetes (ACCORD) trial (described in Chapter 3) was an NHLBI-sponsored 2×2 partial factorial trial comparing intensive (HbA1c < 6.0% target, 6.4% attained) to standard (HbA1c 7.0–7.9% target, 7.5% attained) glycemic control in 10,251 patients with type 2 diabetes who also had either hypertension or metabolic syndrome.28 The primary outcome was all-cause mortality.
• The Action in Diabetes and Vascular Disease: Preterax and Diamicron Modified Release Controlled Evaluation (ADVANCE) trial was an international investigator-initiated trial supported by Servier, the manufacturer of the two preferred drugs used in the trial (gliclazide and a fixed combination of perinodopril and indapamide), which compared intensive (HbA1c <6.5% target, 6.5% attained) versus standard (HbA1c target based on local guidelines, 7.3% attained) in 11,340 patients with type 2 diabetes.29 The primary outcome was the combined incidence of adverse microvascular and macrovascular complications.
• The Veterans Administration Diabetes Trial (VADT) compared intensive versus standard glycemic control in 1791 military veterans (nearly all men) with poorly controlled diabetes and attained HBA1c levels of only 8.4% in the standard group versus 6.9% in the intensive group.30 The primary outcome was a composite of macrovascular complications.
• The Look AHEAD (Action for Health in Diabetes) study was an NIDDK-sponsored multicenter randomized trial of weight loss in 5145 overweight adults with type 2 diabetes.31 The primary outcome was death from cardiovascular causes. The intervention produced an 8.5 kg weight loss and a mean HbA1c of 6.6% (versus 7.2% in the control group) after one year, but neither was sustained.
None of these four studies supported the hypothesis that more intensive glycemic control reduced heart attack, stroke, or other macrovascular events in diabetes. ADVANCE was the only one of the trials that showed a significant reduction in its primary outcome (which included microvascular complications as well as macrovascular events), but this reduction was due entirely to a reduction in microvascular events. Heart attack and mortality rates were no lower in the intensive than the standard group. The results of the ACCORD trial were even worse; the study was stopped early due to excess mortality in the intensive glycemic control group. One problem with trying to lower blood sugar levels aggressively is the risk of overshooting the mark and inducing hypoglycemia (low blood sugar), which can cause fainting, bodily injury, and even death if glucose is not administered promptly. The VADT was badly underpowered and showed no difference in the composite outcome. In the Look AHEAD study, patients in the intervention group quickly regained the weight they lost in Year 1; by the end of the 10-year trial, mean HbA1c was a mere 0.1% lower in the intervention group than in the control group, and of course there was no difference in cardiovascular mortality. Thus, an additional decade of clinical trials had brought us no closer to proving that intensive glycemic control improved heart attack rates or longevity in diabetes than we were in 2000.
Dipeptidyl Peptidase-4 (DPP4) Inhibitors
As the 21st century entered its second decade, a promising new class of diabetes drugs, the DPP4 inhibitors, came on the scene. Like sulfonylureas, they stimulate insulin secretion, but without the undesirable side effect of weight gain.32 Early animal studies showed inhibition of atherosclerosis in rabbits and rodents. However, three large, randomized trials in humans—using saxagliptin (SAVOR), alogliptin (ExAMINE), and sitagliptin (TECOS)—have shown only that these drugs are equivalent to sulfonylureas in reducing adverse cardiovascular events in type 2 diabetes.33
Newer Drugs
Two additional classes of drugs have now been approved for clinical use in type 2 diabetes. the Glucagon–like Peptide-1 (GLP-1) receptor agonists, which include exenatide (which was first identified in gila-monster saliva), liraglutide, and several newer variants, must be injected and are expensive and therefore not widely used.34 The newest drugs, the sodium-glucose cotransporter (SGLT) inhibitors like empaglifozin, dapaglifozin, and canaglifozin, reduce glucose reabsorption by the kidneys and thus increase the level of glucose in the urine while decreasing it in the blood.35 Clinical trial data on long-term cardiovascular effects of these drugs are lacking.
Impact of Advances in Treating Diabetes on the Decline in Cardiovascular Mortality
We have come a long way in improving the lives of persons with diabetes in the past century. The discovery and mass availability of insulin means that they no longer have to worry about having their lives cut short by diabetic ketoacidosis at an early age. The application of clinical trial results showing the benefits of tight glycemic control has meant that most diabetic patients today will not end up like Jackie Robinson—white-haired and nearly blind by age 50 and dead at age 53. However, we still do not have a diabetes drug or combination of drugs that will demonstrably reduce morbidity and mortality from heart attack and stroke. Fortunately, we do have drugs that reduce cardiovascular mortality in diabetics by lowering their blood pressure and their LDL cholesterol.36
However, the bad news is that the prevalence of type 2 diabetes has exploded, especially during the past two decades (Figure 7.1).37
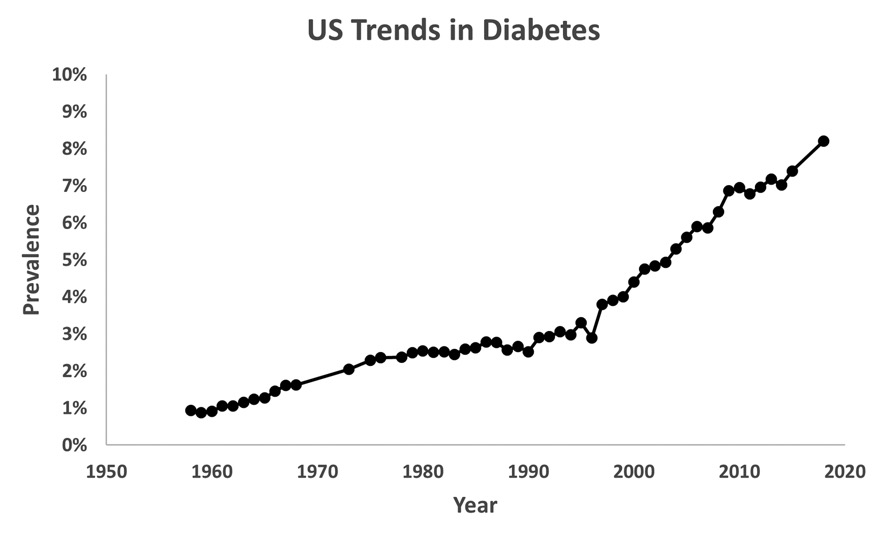
U.S. trends in diabetes, 1958–2015, from CDC data. https://www.cdc.gov/Diabetes/statistics/slides/long_term_trends.pdf
As recently as 1999, the prevalence of diagnosed diabetes in the U.S. was 4.0%. In 2018 (the most recent available data) it was 8.2%. Type 2 diabetes accounts for 90–95% of the disease burden, which is fueled, no doubt, by the rising prevalence of obesity in the U.S. (see Chapter 14). The upward trend shows no signs of abating; if anything, it is growing steeper. And to make matters worse, despite the myriad available treatment options, only 20.9 % of diabetics in 2013–16 were treated and controlled.38 By contrast, 45.2% of diabetics were treated but not controlled, 9.2% were diagnosed but not treated, and 24.7% were not even diagnosed.
Thus, it is evident that the decline in mortality from heart attack and stroke since 1960 has occurred despite, not because of, any progress we have made in controlling diabetes, where advances in treatment have been outstripped by its rising prevalence. Turning once again to the IMPACT model, its estimated 2.9% increase in the prevalence of diabetes between 1980 and 2000 slowed the decline in cardiovascular mortality in this period by 10%.39 And, as we have seen, the prevalence of type 2 diabetes has risen to 8.2% since then.
However, while the rising prevalence of diabetes is a significant problem, its impact to date has not been quite as dire as this model portrays. The model estimates that the 2.9% rise in the prevalence of diabetes from 6.5% in 1980 to 9.5% in 2000 offset 10% of the decline in the annual heart attack mortality rate from 345 to 187 deaths per 100,000 during this period. In other words, were it not for the rise in diabetes, the heart attack mortality rate would have fallen by an additional 12 deaths to 175 deaths per 100,000. However, Ford’s assumed diabetes prevalence rates are far higher the CDC prevalence rates—2.54 and 4.4%, respectively—plotted in Figure 7.1. Therefore, the model’s estimate of the adverse impact of diabetes on heart attack mortality is almost certainly too high. Also, the IMPACT model does not consider any improvements in treatment that may have mitigated this impact either before or after 2000. Although treatments designed to lower HbA1c have not demonstrably altered the fact that diabetics have at three times the risk for heart attacks as non-diabetic, the IMPACT model doesn’t consider the rapidly growing use of statins, which are now given to more than half of all type 2 diabetics and has reduced their heart attack mortality rate (as well as that of non-diabetics) by one-third.40
Therefore, rather than extrapolate the published IMPACT estimate to 2017, I have taken a different approach, which considers the other advances in treatment that have dramatically driven down CHD mortality rates in both diabetics and non-diabetics since 1968 (see the appendix, Table A.5). I have calculated that if the prevalence of diabetes had remained at its 1968 level (1.6%) rather than increasing to 8.2% in 2017, but we still had all the other modern treatments described in other chapters of this book, the CHD mortality rate in 2017 would have fallen by an additional 10.5 deaths to 82.4 deaths per 100,000. This represents an additional 11.3% drop relative to the actual 2017 mortality rate but only 2.2% of the 1968 CHD mortality rate. On the other hand, if the prevalence of diabetics were 8.2% in 1968, there would have been an additional 61.7 CHD deaths per 100,000 that year. Under either scenario, CHD mortality would have fallen by 82.9% rather than 80.7% if the prevalence of diabetes had been unchanged. So the big story is the 80.7% decline in CHD mortality due to treatments that reduced mortality in diabetics and non-diabetics alike, not the extra 2.2% decline we could have realized had the prevalence of diabetes not increased.
However, this is not a call for complacency about the long-term trend in diabetes. The trend line in Figure 7.1 is growing ever steeper and shows no sign of abating. In the meantime, the rate of decline in heart attack has fallen from 38% per 10 years in 2012 to 28% per 10 years in 2017. It is not unreasonable to attribute at least part of this deceleration to the rising tide of diabetes. If the prevalence of diabetes were to continue to climb apace and reaches 40% in the next twenty years or so, I have calculated that the CHD mortality could increase by 55% from 92.7 to 143.7 deaths per 100,000, unless we make major advances elsewhere (see Table A.5 in the appendix). Just as we were in the rising arm of an atherosclerosis pandemic in 1920, we may now be in the rising arm of a diabetes epidemic in the U.S. in 2020. And just as the 20th-century atherosclerosis pandemic rendered the great influenza pandemic of 1918–19 a historical footnote, the gathering 21st-century U.S. diabetes epidemic may be with us long after COVID-19 fades into history.
1. National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK) official website. Health Information/Diabetes. https://www.niddk.nih.gov/health-information/diabetes.
Centers for Disease Control and Prevention (CDC). National Diabetes Statistics Report 2020. Estimates of Diabetes and its Burden in the United States. https://www.cdc.gov/diabetes/pdfs/data/statistics/national-diabetes-statistics-report.Pdf.
2. AM Ahmed. History of Diabetes Mellitus. Saudi Med J 2002; 23:373–378.
3. National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK) official website. Type 1 Diabetes. https://www.niddk.nih.gov/health-information/diabetes/overview/what-is-diabetes/type-1-diabetes.
4. M Bliss. The Discovery of Insulin. Toronto: McClelland & Steward, 1982.
5. NIDDK Type 1 Diabetes.
6. Jackie Robinson at age 53, shortly before his fatal heart attack on October 24, 1972. https://www.ebay.com/i/362305119438?chn=ps&norover=1&mkevt=1&mkrid=711-213727-13078-0&mkcid=2&itemid=362305119438&targetid=4580702888518295&device=c&mktype=&googleloc=&poi=&campaignid=395665092&mkgroupid=1233652256105976&rlsatarget=pla-4580702888518295&abcId=1129776&merchantid=51291&msclkid=8b01eecc521018263cc8b02a2adcb8a8.
7. CDC National Diabetes Statistics Report 2020.
8. National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK) official website. Type 2 Diabetes. https://www.niddk.nih.gov/health-information/diabetes/overview/what-is-diabetes/type-2-diabetes.
9. A Cerami. The unexpected pathway to the creation of the HbA1c test and the discovery of AGE’s. J Intern Med 2012; 271:218–226. Doi: 10.1111/j.1365-2796.2012.02514.x.
10. E Selvin, MW Steffes, H Zhu, K Matsushita, L Wagenknecht, J Panikow, J Coresh, FL Brancati. Glycated hemoglobin, diabetes, and cardiovascular risk in nondiabetic adults. N Engl J Med 2010; 800–811. doi: 10.1056/NEJMoa0908359.
11. Mayo Clinic. Type 2 Diabetes. https://www.mayoclinic.org/diseases-conditions/type-2-diabetes/diagnosis-treatment/drc-20351199.
12. American Diabetes Association. Standards of Medical Care in Diabetes—2018. Diabetes Care 2018; 41 (supplement 1):S1-S159. http://diabetesed.net/wp-content/uploads/2017/12/2018-ADA-Standards-of-Care.pdf.
13. Mayo Clinic..
14. ADA Guidelines 2018, Figure 8.1.
15. ClinCalc DrugStats Database. The top 200 drugs of 2020. https://clincalc.com/DrugStats/Top200Drugs.aspx.
16. University of Minnesota Driven to Discover. Heart Attack Prevention. The University Group Diabetes Program (UGDP): A famous early randomized clinical trial (RCT). http://www.epi.umn.edu/cvdepi/essay/the-university-group-diabetes-program-ugdp-a-famousearly-randomized-clinical-trial-rct/.
17. TB Schwartz and CL Meinert. The UGDP controversy: Thirty-four years of contentious ambiguity laid to rest. Perspect Biol Med 2004; 47:564–574.
18. LA Conlay, JE Loewenstein. Phenformin and Lactic Acidosis. JAMA 1976; 235:1575–1578. doi:10.1001/jama.1976.03260410031019.
19. The Diabetes Control and Complications Trial Research Group. The effect of intensive treatment of diabetes on the development and progression of long-term complications in insulin-dependent diabetes mellitus. N Engl J Med 1993; 329:977–986.
20. P Reichard, BY Nilsson, U Rosenqvist. The effect of long-term intensified insulin treatment on the development of microvascular complications of diabetes mellitus. N Engl J Med 329: 304–309.
Y Ohkubo, H Kishikawa, E Araki, Y Kojima, N Furuyoshi, M Shichiri. Intensive insulin therapy prevents the progression of diabetic microvascular complications in Japanese patients with non-insulin dependent diabetes mellitus: a randomized prospective 6-year trial. Diab Res Clin Pract 1995; 28:103–117. https://www.diabetesresearchclinicalpractice.com/article/0168-8227(95)01064-K/pdf.
21. UK Prospective Diabetes Study (UKPDS) Group. Intensive blood-glucose control with sulphonylureas or insulin compared with conventional treatment and risk of complications in patients with type 2 diabetes (UKPDS 33). Lancet 1998; 352:837–853.
22. UK Prospective Diabetes Study (UKPDS) Group. Effect of intensive blood-glucose control with metformin on complications in overweight patients with type 2 diabetes (UKPDS 34). Lancet 1998; 352:854–865.
23. P King, I Peacock, R Donnelly. The UK Prospective Diabetes Study (UKPDS): clinical and therapeutic implications for type 2 diabetes. J Clin Pharmacol 1999; 48:643–649.
24. PD Home, SJ Pocock, H Beck-Nelson, R Gomis, M Hanefeld, NP Jones, M Komajada, JJV McMurray, for the RECORD Study Group. Rosiglitazone evaluated for cardiovascular outcomes—an interim analysis. N Engl J Med 2007; 357:28–38.
25. The BARI-2D Study Group. A randomized trial of therapies for type 2 diabetes and coronary artery disease. N Engl J Med 2009; 360:2503–2515.
26. JA Dormandy, B Charbonel, DJA Eckland, E Erdman, M Massi-Benedetti, IK Moules, MH Tan, PJ Lefebvre, GD Murray, E Standl, RG Wilcox, L Wilhelmsen, J Betteridge, K Birkeland, A Golay, RJ Heine, L Koranyi, M Laakso, M Mokan, A Norkus, V Pirags, T Podar, A Scheen, W Scherbaum, G Schernthaner, O Schmitz, J Skrha, U Smith, J Taton, on behalf of the PROActive Investigators. Secondary prevention of macrovascular events in patients with type 2 diabetes in the PROactive Study (PROspective pioglitzAzone Clinical Trial In macrovascular Events): a randomized controlled trial. Lancet 2005; 366:1279–1289. DOI: https://doi.org.10.1016/S0140-6736(05)67528-9.
27. S Singh, YK Loke, CD Furberg. Long-term risk of cardiovascular events with rosiglitazone: a meta-analysis. JAMA 2007; 298:1189–1195.
28. The Action to Control Cardiovascular Risk in Diabetes Study Group. Effects of intensive glucose lowering in type 2 diabetes. N Engl J Med 2008; 358:2545–2559.
29. The ADVANCE Collaborative Group. Intensive blood glucose control and vascular outcomes in patients with type 2 diabetes. N Engl J Med 2008; 358: 2560–2572.
30. W Duckworth, C Abraira, T Moritz, D Reda, N Emanuele, PD Reaven, FJ Zieve, J Marks, SN Davis, R Hayward, SR Warren, S Goldman, M McCarren, ME Vitek, WG Henderson, GD Huang, for the VADT Investigators. Glucose control and vascular complications in veterans with type 2 diabetes. N Engl J Med 2009; 360:129–139.
31. The Look AHEAD Research Group. Cardiovascular effects of intensive lifestyle intervention in type 2 diabetes. N Engl J Med 2013; 369:145–154.
32. J Zhong, S Kankanala, S Rajagopalan. DPP4 inhibition: insights from the bench and recent clinical studies. Curr Opin Lipidol 2016; 27:484–492. doi: 10.1097/MOL.0000000000000340.
33. BM Scirica, DL Bhatt, E Braunwald, PG Steg, J Davidson, B Hirshberg, P Ohman, R Frederich, SD Wiviott, EB Hoffman, MA Cavender, JA Udell, NR Desai, O Mozenzon, DK McGuire, KK Ray, LA Leiter, I Raz, for the SAVOR-TIMI-53 Steering Committee and Investigators. Saxagliptin and cardiovascular outcomes in patients with type 2 diabetes mellitus. N Eng J Med 2013; 369:1317–1326. DOI: 10.1056/NEJMoa1307684.
WB White, CP Cannon, SR Heller, SE Nissen, RM Bergenstal, GL Bakris, AT Perez, PR Fleck, CR Mehta, S Kupfer, C Wilson, WC Cushman, F Zannad, for the Examine Investigators. Alogliptin after acute coronary syndrome in patients with type 2 diabetes. N Engl J Med 2013; 369:1327–1335. DOI: 10.1056/NEJMoa1305889.
JB Green, MA Bethel, PW Armstrong, JB Buse, SS Engel, J Garg, R Josse, KD Kaufman, J Koglin, S Korn, KM Lachin, DK McGuire, MJ Pencina, E Standl, PP Stein, S Suryawanshi, F Van de Werf, ED Peterson, RR Holman, for the TECOS Study Group. Effect of sitagliptin on cardiovascular outcomes in type 2 diabetes. N Engl J Med 2015; 373:232–242. DOI: 10.1056/NEJMoa1501352.
34. AJ Garber. Long-acting glucagon-like peptide 1 receptor agonists: a review of their efficacy and efficiency. Diabetes Care 2011; 34:S279-S284.
35. DS Hsia, O Grove, WT Cefalu. An update on SGLT2 inhibitors for the treatment of diabetes mellitus. Curr Opin Diabetes Obes 2017; 24:73–79.
36. JD Curb, SL Pressel, JA Cutler, PJ Savage, WB Applegate, H Black, G Carmel, BR Davis, PH Frost, N Gonzalez, G Guthrie, A Oberman, GH Rutan, J Stamler, for the Systolic Hypertension in the Elderly Program Cooperative Research Group. Effect of diuretic-based antihypertensive treatment on cardiovascular disease risk in older diabetic patients with isolated systolic hypertension. JAMA 1996; 276:1896–1892.
Cholesterol Treatment Trialists Collaboration. Efficacy of cholesterol-lowering therapy in 18,686 people with diabetes in 14 randomised trials of statins: a meta-analysis. Lancet 2008; 371:117–125.
37. CDC’s Division of Diabetes Translation. United States Diabetes Surveillance System. Long-term Trends in Diabetes April 2017. https://www.cdc.gov/Diabetes/statistics/slides/long_term_trends.pdf.
CDC National Diabetes Statistical Report 2020. Estimates of Diabetes and its Burden in the United States. https://www.cdc.gov/diabetes/pdfs/data/statistics/national-diabetes-statistics-report.pdf.
38. A report from the American Heart Association. AHA Statistical Update Heart Disease and Stroke Statistics—2020 Update, Chapter 9: Diabetes Mellitus, Chart 9.6. Circulation 2020; 141:e139-e596. See p. e275. DOI: 10.1161/CIR.0000000000000757.
39. ES Ford, UA Ajani, JB Croft, JA Critchley, DR Labarth, TE Kottke, WH Giles, S Capewell. Explaining the Decrease in U.S. Deaths from Coronary Disease, 1980–2000. N Engl J Med 2007; 356:2388–2398. DOI: 10.1056/NEJMsa053935.
40. JA Salami, H Warralch, J Velardo-Elizondo, ES Spatz, NR Desai, JS Rana, SS Virani, R Blankstein, A Khera, MJ Blaha, RS Blumenthal, D Lloyd-Jones, K Nasir. National trends in statin use and expenditures, in the U.S. adult population from 2002 to 2013: Insights from the Medical Expenditure Panel survey. JAMA Cardiology 2017; 2:56–65. doi.10.1001/jamacardio.2016.4700. Cholesterol Treatment Trialists Collaboration.