6
The story of the third potentially reversible Framingham cardiovascular risk factor, cigarette smoking, differs importantly from that of hypertension and high cholesterol in that cigarette smoke was already a proven carcinogen by the time the first Framingham results were reported in 1961. Therefore, efforts to control this risk factor were always a matter of changing public opinion and behavior more than proving that smoking caused heart disease. Furthermore, cardiovascular public health scientists took a back seat to specialists in lung disease and cancer in these efforts. Although the public sector, specifically the Surgeon General’s office and the Centers for Disease Control and Prevention (CDC), played an important coordinating role, these efforts were spearheaded in the U.S. by national and local chapters of volunteer organizations like the American Lung Association (ALA), the American Cancer Society (ACS), and the American Heart Association (AHA).
The major epidemiologic studies of smoking were done in the early 1950s by Richard Doll and Bradford Hill in the UK and by Cuyler Hammond and Daniel Horn in the U.S.1 In their landmark 1952 retrospective case-control study, in which men comprised 93% of all cases, Doll and Hill found that only seven of 1357 men with lung cancer (0.5%) versus 61 male controls (4.5%) were non-smokers.2 There was a strong graded dose-response relationship, with lung cancer rates at least 10 times higher in heavy smokers than in non-smokers. The strong relationship between smoking and lung cancer was confirmed prospectively in 1954 by Doll and Hill in male physicians and in a larger ACS-supported U.S. study by Hammond and Horn in 187,766 50- to 69-year-old men.3 By 1964, when the U.S. Surgeon General issued the historic report of his advisory committee on smoking health, implicating smoking in chronic obstructive lung disease and cardiovascular disease, as well as lung cancer, randomized trials of smoking were no longer ethically viable.4
Although tobacco has been with us since colonial times, cigarettes are a relatively recent phenomenon. Before 1900, most tobacco was either chewed or smoked in pipes and cigars, which because they tend to be consumed in modest amounts and their smoke is not deeply inhaled, are less addictive and less damaging to the lungs.5 Annual per capita cigarette consumption in 1900 was only 54 cigarettes.6 Lung cancer was quite rare. The development of technology for the mass production of inexpensive cigarettes circa 1900 changed all this. Per capita cigarettes in the U.S. rose almost 100-fold to 4345 cigarettes per adult per year in 1965, when 42.4% of Americans smoked them. By 1950, consumption, which comprised less than 1% of American tobacco consumption in 1880, accounted for 80% of American tobacco consumption. Lung cancer had become the leading cause of cancer death in American men in 1954, and surpassed breast cancer as the leading cause of cancer death in American women in 1987.
The prevalence of cigarette smoking in U.S. adults has declined steadily from the early 1960s to the present (Figure 6.1A), reaching a new low of 13.7% in 2018 (Figure 6.1A).7
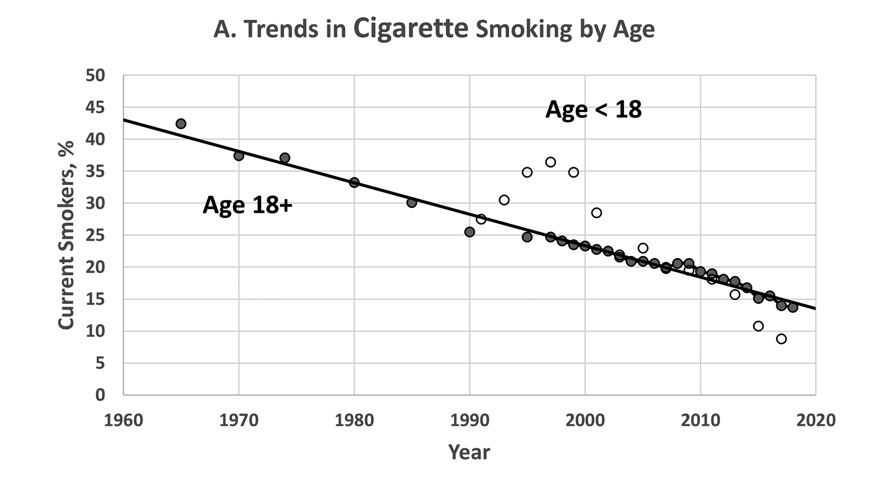
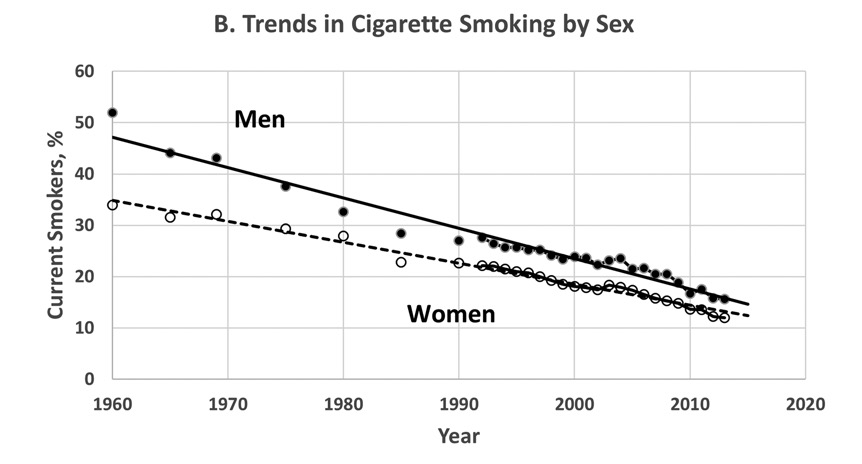
U.S. trends in cigarette smoking, 1960–2018, from the American Lung Association website. Trends are shown by age group (Figure 6.1A) and sex (Figure 6.1B).
The prevalence of cigarette smoking among youths under age 18 surged briefly in the 1990s but is now less than that in adults, although this trend has been more than offset by the rising popularity of electronic cigarettes.8 Cigarette smoking has always been more prevalent in men than women but has declined more rapidly in men, and the gender gap has steadily declined from almost 30% in the mid–1950s to 3.6% in 2018 (Figure 6.1B).
Lung cancer mortality (which reflects the long-term, largely irreversible ravages of smoking on lung tissue) has been falling since 1993, lagging almost 30 years behind the decline in cigarette smoking, with annual declines of 1.9% in men and 0.9% in women.9 The rise and decline in cigarette smoking closely parallels the trend in heart attack mortality (Figure 1.1), covering the same period. In contrast to lung cancer, there is no perceptible lag time behind the trend in smoking, because the cardiovascular effects of smoking tend to be acute and mostly reversible—if a person stops smoking.
This chapter will address three questions:
1. How did cigarettes become so popular?
2. How was the post–1963 decline in cigarette smoking achieved?
3. To what extent do the rise and decline in smoking from 1900–2020 explain the trends in mortality from heart attacks, strokes, and other cardiovascular causes?
The rise in the popularity of smoking in 1900–60 was fueled largely by changes in the tobacco curing process, producing a sweeter, milder blend, the portability and affordability of cigarettes, and the invention of safety matches. But cigarettes were also heavily marketed by direct advertising and by what would now be called “product placement” in movies and other popular entertainments. Cigarette smoking was popularly portrayed as relaxing and soothing, endorsed by doctors and celebrities; you can check out some of the more absurd examples on the internet.10 They were endorsed by celebrities like Lucille Ball, Gary Cooper, Arthur Godfrey, and Steve McQueen. They were even marketed to women as a means of weight control, as in “Reach for a Lucky instead of a sweet” and (if you can believe it) as a remedy for the symptoms of asthma, bronchitis, and influenza. Although cigarette sales took a hit during the Great Depression and again in the early 1950s, following the studies linking smoking and lung cancer, tobacco companies countered by marketing filter cigarettes and other brands with reduced tar and nicotine content and/or menthol. Cigarette consumption quickly rebounded. By 1960, half of all cigarettes smoked in the U.S. had filters.11 But new ads like those featuring a rugged cowboy called “the Marlboro Man” and an ad for a new cigarette brand for women called Virginia Slims (“You’ve come a long way, baby!”) were still all over television in the 1960s. Pioneering newscaster John Cameron Swayze sat in front of a Camels logo on his daily newscasts, and the main characters in popular TV shows of the era (like Perry Mason) smoked cigarettes. In this environment, the 1964 Surgeon General’s report exploded like a bombshell, creating a huge flurry of headlines and rating among the top news stories of 1964.12 However, all this publicity made only a small dent in cigarette consumption.
Following the Surgeon General’s report, the U.S. Congress passed two major pieces of anti-smoking legislation.13 The Federal Cigarette Labeling and Advertising Act of 1965 required tobacco companies to put health warnings on all cigarette packaging and to air public service announcements publicizing the deleterious effects of smoking on health. The Public Health Cigarette Smoking Act of 1969 went a step further and banned all cigarette advertising in the broadcast media. However, these new laws did nothing to prevent tobacco companies from rechanneling their advertising budget into print advertising, billboards, etc. In 1975, five years after Richard Nixon signed the cigarette advertising ban into law, per capita cigarette consumption still hovered around 4000 per year, down only about 7% from its peak of 4300 in the early 1960s. Clearly, a broader grass-roots anti-smoking campaign was needed.
One offshoot of the 1964 Surgeon General’s report was the establishment of the National Clearinghouse for Smoking and Health to track the progress of antismoking efforts. This organization soon evolved into the CDC Office on Smoking and Health, which coordinates with national volunteer health organizations like the ALA, ACS, and AHA and their local chapters to support state and community anti-smoking programs, promote tobacco research, and ensure the public visibility of antismoking messaging. It is these grass-roots efforts, which focused on making cigarettes unappealing and curtailing and eventually banning smoking from public spaces, that finally sent per capita cigarette consumption plummeting by more than half during the last quarter of the 20th century. An important driver of these efforts was research on the adverse impact of secondhand smoke on non-smokers, especially children with asthma and other respiratory disorders.14 Although secondhand smoke accounts for a relatively small number of lung cancers, the exacerbation of asthma and other lung conditions in children chronically exposed to tobacco smoke was for more pervasive and alarming. With this new evidence in hand, smoking cigarettes now could be said to involve more than a risky personal lifestyle choice; it also claimed the most innocent of victims.
In 1975, one could expect to be exposed to secondhand cigarette smoke at work, in bars and restaurants, on airplanes and trains, and in hotels. When I sat in a non-smoking section on a flight to Europe in 1973, the smoking section was right across the aisle, about two feet away. Efforts to change this culture began modestly with local campaigns—like a successful effort by the local chapter of the AHA in my hometown of Chicago in the late 1970s to persuade local restaurant associations to call for designated non-smoking sections in restaurants. Then, these efforts began gradually to pick up steam Some important landmarks in this battle are listed below:
Table 6.1 Anti-Smoking Landmarks, 1975–200015
|
1975 |
Minnesota becomes the first state to require separate smoking areas in public places by passing the Minnesota Clean Indoor Air Act. |
|
1984 |
The USFDA approves nicotine gum as the first drug designed to help people quit smoking. |
|
1986 |
A new Surgeon General’s report on the Health Consequences of Involuntary Smoking is issued, emphasizing the harmful effects of secondhand smoke.16 A final definitive report was issued in 2006. |
|
1987 |
Congress prohibits smoking on short domestic flights. Before this, smoking was allowed in the back rows of domestic flights. |
|
1987 |
Aspen, Colorado, becomes the first city in the U.S. to require smoke-free restaurants. |
|
1988 |
California voters approve Proposition 99, which imposed a 25% surtax on cigarettes and earmarked the additional revenue to create a statewide anti-tobacco control program. |
|
1988 |
American Lung Association, American Heart Association and American Cancer Society establish Tobacco Free America to publish “State Legislated Actions on Tobacco Issues,” which tracks relevant taxes, laws, and programmatic funding for every state.17 |
|
1989 |
Congress bans smoking on all domestic airlines. |
|
1990 |
San Luis Obispo becomes the first city to ban smoking in all public buildings, including bars and restaurants. |
|
1993 |
The U.S. Environmental Protection Agency published a report concluding that secondhand smoking is responsible for approximately 3000 lung cancer deaths annually in nonsmoking adults and respiratory impairment in hundreds of thousands of children.18 |
|
1998 |
California becomes the first state to issue a comprehensive ban of smoking in all bars and restaurants. |
|
1998 |
Attorneys General from 46 states reach a multibillion dollar damages settlement with tobacco industry. |
|
1999 |
The U.S. Department of Justice sues the tobacco industry under the RICO (racketeering) statute, claiming that they engaged in “a coordinated campaign of fraud and deceit.” This lawsuit was decided in the government’s favor in 2006. |
Restrictions on smoking have continued to grow in the 21st century, and the prevalence of smoking has continued to fall, reaching a new low of 13.7% in 2018.19
The success of anti-smoking efforts has been predominantly in encouraging smokers to give up the habit, rather than preventing teenagers and young adults from acquiring it. The proportion of “ever-smokers” who have quit smoking has increased at a steady pace from 24.2% in 1965 to 61.7% in 2018.20 By contrast, the proportion of 12- to 17-year-olds who start smoking rose from 12% in the mid–1960s to as high 16% a decade later, then fell back to 12% in the late 1980s and early 1990s, rose again to 14% in the late 1990, and fell to 11% in 2002–03.21 The trend in 18- to 25-year-olds is somewhat more encouraging, falling from a high of 11% in 1968 to below 6% in the early 1980s and rebounding slightly to 7% in 2000–03.22 However, more recently, starting in 2007, a new phenomenon—electronic cigarettes (e-cigarettes) or “vaping”—has taken hold among adults seeking a “safer” alternative to smoking and, more ominously, among teenagers, who are attracted to their candy-like flavors. While e-cigarette use has remained steady at roughly 3% in adults, there has been an alarming two-year increase in their use in high schoolers (11.7% in 2017 to 27.5% in 2019) and in middle schoolers (3.3% in 2017 to 10.5% in 2019).23 Because of this sharp uptick in e-cigarette use, nearly one in three high-schoolers and one in eight middle-schoolers used some form of tobacco in 2019. While vaping may not deliver carcinogenic tars into the lungs, it does effectively deliver nicotine with its associated risk for cardiovascular disease and acute asthmatic attacks and is just as addictive as tobacco. In 2019, there were sporadic reports of unusual acute (and even fatal) respiratory distress syndrome in young consumers of flavored e-cigarettes and calls for banning these products.24
Cardiovascular Impact of Trends in Smoking
There is no doubt that the marked decline in cigarette consumption and in prevalence of smoking from 42% in 1965 to 14% in 2018 has saved millions of American lives and has extended life expectancy. Holford et al. calculated that the reduction in smoking between 1964 and 2012 increased life expectancy by 2.3 years in men and 1.6 years in women and has resulted in 157 million years of life saved.25 These gains in life expectancy represent just under 30% of the observed 7.8- and 5.4-year overall gains during this 48-year period in men and women, respectively. Reducing cigarette smoking, which has reduced incidence of and mortality from lung and other cancers and chronic obstructive lung disease, as well as cardiovascular disease, is probably the single most impactful public health accomplishment of the last half of the 20th century.
But in keeping with the object of this book, let us focus more narrowly on the role of the anti-smoking effort in quelling the cardiovascular pandemic of the 20th century. The IMPACT model estimates that the decline in cigarette smoking was responsible for 11.7% of the 46% decline in heart attack mortality between 1980 and 2000.26 Given the fact that the decline in cigarette smoking from 40% in 1968 to 14% in 2017 was 2.57 times as great as the decline from 33% in 1980 to 23% in 2000, this extrapolates to smoking cessation accounting for 16.4% of the 81% decline in heart attack mortality since 1968 (see the appendix, Table A.2).
One can apply the same approach to extrapolate the published IMPACT results of 1980–2000 back in time to analyze the contribution of cigarettes to the onset of the cardiovascular pandemic. In contrast to BP and cholesterol, we have reliable cigarette consumption data going back to 1900, when cigarette smoking first became popular (Figure 6.1). We must make two modifications:
1. Lacking national heart attack mortality data before 1950, we must base the analysis on the decline in heart disease mortality, which includes cardiomyopathy, rheumatic, congenital, hypertensive and other heart conditions, as well as heart attacks.
2. Ford et al. relied on non-randomized studies of smoking cessation, in which heart attack risk was reduced by 36%, rather than the roughly 50% reduction one would expect if heart attack risk returned to its pre-smoking baseline.27 While this assumption is defensible in analyzing the decline in smoking since 1968 (which was driven by smoking cessation rather than preventing new smokers), it is clearly not valid when analyzing the rise in smoking between 1900 and 1968, in which each new smoker can be more reasonably assumed to have doubled his/her heart attack risk.28
After making these adjustments, I have estimated that the rise in smoking prevalence from 0 in 1900 to nearly 40% in 1968, accounted for nearly 28% of the 100% increase in heart disease mortality from 265.4 to 531.0 deaths per 100,000 between 1900 and 1968 (see the appendix, Table A.3). The contribution might be even larger if one assumes that cigarette smoking more than doubles the risk of a heart attack. Efforts to discourage teenagers and young adults from smoking may hold the key to further progress, although their short-term cardiovascular risk is low.
1. JM Samet, FE Speizer. Sir Richard Doll, 1912–2005 (obituary). Am J Epidiol 2006; 164:95–100.
2. R Doll, AB Hill. A study of the aetiology of carcinoma of the lung. Br Med J 1952; 2:1271–1286.
3. R Doll R, AB Hill. The mortality of doctors in relation to their smoking habits. A preliminary report. BMJ 1954; 228(i):1451–55. EC Hammond, D Horn. The relationship between human smoking habits and death rates: A follow-up study of 187,766 men. JAMA 1954; 155:1316–1328. doi:10.1001/jama.1954.03690330020006.
4. L Terry, et al. Smoking and Health: Report of the Advisory Committee to the Surgeon General of the United States. U-23 Department of Health, Education, and Welfare. Public Health Service Publication No. 1103. 1964 https://profiles.nlm.nih.gov/spotlight/nn/catalog/nlm:nlmuid-101584932X202-doc.
5. Epidemiology of Tobacco Use: History and Current Trends. https://www.nap.edu/read/11795/chapter/4.
6. CDC MMMR Weekly. 1999 Tobacco Use—United States, 1900–1999. November 5, 1999; 48:986–993. https://www.cdc.gov/mmwr/preview/mmwrhtml/mm4843a2.htm.
7. American Lung Association. Overall Tobacco Trends. https://www.lung.org/research/trends-in-lung-disease/tobacco-trends-brief/overall-tobacco-trends. Accessed October 2020.
8. Ibid.
9. CA Ridge, AM McErlean, MS Ginsberg. Epidemiology of lung cancer. Semin Intervent Radiol 2013; 30:93–98.
10. Absurd Old Smoking Ads. https://www.google.com/search?q=absurd+old+smoking+ads&tbm=isch&client=firefox-b-1-d&hl=en&ved=2ahUKEwimp7H1l-vpAhWHON8KHRjeDHwQrNwCKAF6BQgBEOIB&biw=773&bih=560.
11. Epidemiology of Tobacco Use.
12. Centers for Disease Control and Prevention. Smoking & Tobacco Use: A Brief History. https://www.cdc.gov/tobacco/data_statistics/sgr/history/index.htm.
13. A Glass. Congress bans airing cigarette ads. April 1, 1970. https://www.politico.com/story/2018/04/01/congress-bans-airing-cigarette-ads-april-1-1970-489882.
14. A report of the Surgeon General. The Health Consequences of Involuntary Exposure to Tobacco Smoke. Centers for Disease Control and Prevention (U.S.), Atlanta, GA, 2006. https://www.ncbi.nlm.nih.gov/books/NBK44324/.
15. American Lung Association. Tobacco Control Milestones. https://www.lung.org/research/sotc/tobacco-timeline.
16. Centers for Disease Control. 1986 Surgeon General’s Report: The Health Consequences of Involuntary Smoking. MMWR Morb Mortal Wkly Rep 1986; 35:769–70. PMID 3097495.
17. State Legislated Actions on Tobacco Issues (SLATI). https://www.lung.org/policy-advocacy/tobacco/slati.
18. EPA. Respiratory Health Effects of Passive Smoking: Lung Cancer and Other Disorders. Office of Health and Environmental Assessment, Office of Research and Development, U.S. Environmental Protection Agency, Washington, DC, December 1992.
19. C Crawford. Cigarette smoking among U.S. adults hits an all-time low. AAFP News. November 20, 2019. https://www.aafp.org/news/health-of-the-public/20191120mmwr-cigarettesmoking.html.
20. American Lung Association. Overall Tobacco Trends.
21. Epidemiology of Tobacco Use. Figure 1.4.
22. Ibid.
23. American Lung Association. Overall Tobacco Trends.
U.S. Food and Drug Administration. 2018 National Youth Tobacco Survey Finds Cause for Concern. https://www.fda.gov/tobacco-products/youth-and-tobacco/2018-nyts-data-startling-rise-youth-e-cigarette-use.
24. Centers for Disease Control and Prevention. Surgeon General’s Advisory on E-cigarette Use Among Youth. February 2020. https://www.cdc.gov/tobacco/basic_information/e-cigarettes/surgeon-general-advisory/index.html.
25. TR Holford, R Meza, KE Warner, C Meernik, J Jeon, SH Moolgavkar, DT Levy. Tobacco Control and the Reduction in Smoking-Related Premature Deaths in the United States, 1964–2012. JAMA 2014; 311(2):164–171. doi:10.1001/jama.2013.285112.
26. ES Ford, UA Ajani, JB Croft, JA Critchley, DR Labarth, TE Kottke, WH Giles, S Capewell. Explaining the Decrease in U.S. Deaths from Coronary Disease, 1980–2000. N Engl J Med 2007; 356:2388–2398. DOI: 10.1056/NEJMsa053935.
27. JA Critchley, S Capewell. Mortality risk reduction associated with smoking cessation in patients with coronary heart disease: a systematic review. JAMA 2003; 290:86–97. Doi: 10.1001/jama.290.1.86.
28. AHA/ACC Heart Risk Calculator, http://www.cvriskcalculator.com/.